
Vitamin K Deficiency: Symptoms, Causes, Treatment, and Prevention; Vitamin K Deficiency Bleeding in Newborns; Warfarin; The Complete Doctor’s Guide.
The vitamin that stops your blood from bleeding and why a single injection at birth prevents a tragedy.
✍️ Written and Reviewed by: Prof. Dr. Qazi Taqweemulhaq, FCPS Medicine. Professor of Medicine, Women Medical and Dental College, Abbottabad, Pakistan. Consultant Physician with 32 Years of Clinical Experience. 📅 Last Updated: June 2026 | References: NIH ODS, NCBI StatPearls, Endocrine Society 2024, NEJM VITAL Trial, Cleveland Clinic, Merck Manual
⚡ Quick Answer: Vitamin K deficiency symptoms include impaired blood clotting — leading to easy bruising, prolonged bleeding, and in newborns, life-threatening VKDB (Vitamin K Deficiency Bleeding) including intracranial haemorrhage. Without prophylaxis, the VKDB risk is 1,700 per 100,000 infants; a single IM injection at birth reduces this to 1 per 100,000. Warfarin works by blocking Vitamin K — understanding this relationship is essential for reversal. Beyond clotting, Vitamin K2 activates proteins for bone mineralisation and arterial calcification prevention. Treatment: phytomenadione (Vitamin K1) orally, IV, or IM — with PCC for emergency warfarin reversal.
✅ KEY TAKEAWAYS – Vitamin K Deficiency |
• Vitamin K is required to activate coagulation factors II, VII, IX, and X: deficiency causes uncontrolled bleeding that cannot stop without treatment. |
• VKDB (Vitamin K deficiency bleeding) in newborns is the most dangerous consequence; the risk is 1,700 per 100,000 infants without prophylaxis and falls to 1 per 100,000 with a single IM vitamin K injection at birth. |
• Warfarin works by blocking vitamin K. Understanding this relationship explains both how warfarin works and how to reverse its effects |
• Vitamin K deficiency in adults is rare from diet alone. It almost always indicates fat malabsorption, liver disease, antibiotic disruption of gut flora, or drug interference |
• Beyond clotting, Vitamin K2 activates osteocalcin for bone mineralisation and matrix Gla protein for arterial calcification prevention. Deficiency contributes to both osteoporosis and cardiovascular disease |
• Vitamin K1 (phylloquinone) comes from plant foods, especially dark green leafy vegetables. Vitamin K2 (menaquinone) comes from fermented foods and gut bacteria. |
A Baby Who Bled — And the Single Injection That Could Have Prevented It All
The mother was 24 years old. She had delivered a healthy baby boy at home where a routine newborn injection was not given. Her baby was healthy. Breastfeeding had started well.
On day 19 of life, the baby became suddenly irritable and stopped feeding. Within hours, he developed seizures. By the time he reached the emergency department, he was unconscious. His fontanelle was bulging, tense as a drum. The CT scan showed massive bilateral intracranial haemorrhage.
His blood would not clot. His PT was unmeasurable. His INR was greater than 10. He had late Vitamin K Deficiency Bleeding — the form that strikes exclusively breastfed infants who did not receive Vitamin K prophylaxis at birth. The form that, as the CDC states, in the majority of cases gives no warning signs before a life-threatening event begins.
We gave IV Vitamin K and fresh frozen plasma. The seizures stopped. But the damage was done. A child who would have been perfectly healthy, who would have grown and laughed and learned, left that hospital with permanent, life-altering brain damage.
The injection he did not receive costs pennies. Takes seconds. Has been given to virtually every newborn in the developed world for decades. And the Medscape data (August 2025) is unambiguous: the risk of VKDB without prophylaxis is 1,700 per 100,000 infants. With IM Vitamin K at birth, it falls to 1 per 100,000.
This is the story of Vitamin K — the vitamin that activates the proteins your blood needs to clot, that protects your bones from crumbling, and that prevents calcium from silently hardening your arteries. It is also the story of warfarin — one of the world’s most prescribed drugs — which works entirely by blocking Vitamin K, and whose excess dosing or drug interactions can reproduce every feature of Vitamin K deficiency.
🏥 From My Clinic: A 67-year-old man with atrial fibrillation on warfarin came to me with progressive bruising across his abdomen and flanks. His INR was 8.2, more than double the therapeutic range. He had started a 10-day course of ciprofloxacin for a urinary tract infection five days earlier and nobody had warned him about the interaction. Fluoroquinolones kill gut bacteria that produce Vitamin K2, simultaneously dramatically potentiating warfarin’s anticoagulant effect. We withheld warfarin, gave oral Vitamin K 5 mg, and his INR normalised within 48 hours without any active bleeding. He was fortunate. The interaction is well-known, well-documented, and entirely preventable with appropriate counselling.
What Is Vitamin K and What Does It Do?
Vitamin K is a fat-soluble vitamin that exists in two primary dietary forms with overlapping but distinct biological roles. The name derives from the Danish/German word Koagulation, clotting, reflecting its discovery as the essential factor for blood coagulation.
Its mechanism of action is specific and elegant: Vitamin K is the essential cofactor for gamma-glutamyl carboxylase (GGCX)—the enzyme that adds a carboxyl group to glutamate residues on specific proteins. This carboxylation creates calcium-binding sites on those proteins, which are essential for their biological function. Without vitamin K, these proteins are synthesised but remain biologically inactive.
The Vitamin K-Dependent Proteins; A Family With Two Functions
Coagulation Proteins (Vitamin K1 — primary activator)
- Prothrombin (Factor II): central to the clotting cascade, converts fibrinogen to fibrin (the clot)
- Factor VII: triggers the extrinsic coagulation pathway.
- Factor IX: participates in the intrinsic pathway.
- Factor X: converging point of both pathways, activates prothrombin.
- Protein C and Protein S: anticoagulant proteins inactivate Factors Va and VIIIa to prevent excessive clotting.
- Protein Z: inhibits Factor Xa
Vitamin K deficiency impairs ALL of these — creating a complex coagulopathy where both procoagulant factors AND anticoagulant proteins are deficient. In practice, the procoagulant deficit dominates — producing a bleeding tendency
Non-Coagulation Proteins (Vitamin K2 — primary activator)
- Osteocalcin: secreted by osteoblasts — after Vitamin K2 carboxylation, binds calcium in bone matrix. Deficiency impairs bone mineralisation → reduced bone density → osteoporosis
- Matrix Gla Protein (MGP): expressed in vascular smooth muscle — after carboxylation, inhibits calcium deposition in arterial walls. Deficiency → uncontrolled vascular calcification → arterial stiffness → cardiovascular disease
- Gas6: regulates cell survival, proliferation, and immune function
Clinical Insight: Matrix Gla Protein is the most potent known inhibitor of vascular calcification. Vitamin K2 deficiency — independent of K1 deficiency — allows uncontrolled calcium deposition in arterial walls, contributing to the hardening and stiffening of arteries. This explains the growing clinical interest in Vitamin K2 supplementation for cardiovascular and bone health — beyond its role in coagulation.
The Vitamin K Cycle — How the Body Recycles It
Vitamin K is unusual in that the body recycles it efficiently through the Vitamin K epoxide cycle:
- Vitamin K (quinone) is reduced to Vitamin K hydroquinone — the active cofactor for GGCX
- After carboxylation, Vitamin K is oxidised to Vitamin K epoxide
- Vitamin K epoxide reductase (VKOR) converts epoxide back to quinone — ready for reuse
- Warfarin blocks VKOR — interrupting recycling and causing functional Vitamin K deficiency regardless of dietary intake
Vitamin K1 vs Vitamin K2; The Critical Clinical Difference
Understanding the distinction between K1 and K2 is essential for both clinical management and patient counselling:
Feature | Vitamin K1 (Phylloquinone) | Vitamin K2 (Menaquinone) |
Primary source | Dark green leafy vegetables (spinach, kale, broccoli); vegetable oils | Fermented foods (natto, cheese, fermented soya); animal liver; gut bacteria synthesis |
Primary function | Activation of coagulation factors II, VII, IX, X, and Proteins C, S, Z | Activation of osteocalcin (bone mineralisation) and matrix Gla protein (arterial calcification prevention) |
Half-life | Short, hours to 1–2 days | Longer, days to weeks (varies by MK subtype) |
Clinical use | Correcting coagulopathy; reversing warfarin; neonatal prophylaxis | Osteoporosis prevention; cardiovascular calcification prevention; emerging therapeutic use |
Interaction with warfarin | Direct antagonism, K1 restores clotting factor activation blocked by warfarin | Less interaction with warfarin anticoagulation, does not substantially alter INR |
Table 1. Vitamin K1 vs K2 — clinical comparison. Sources: NIH ODS; PMC Ann Lab Med Jul 2025; Merck Manual.
💊 Which Form for Which Purpose: For correcting coagulopathy or reversing warfarin, use Vitamin K1 (phytomenadione). For bone health and arterial calcification prevention, Vitamin K2 (particularly MK-7, the long-chain menaquinone) is the preferred form. The two forms are not interchangeable for these clinical purposes.
How Much Vitamin K Do You Need Per Day?
Vitamin K requirements are expressed as Adequate Intake (AI) — no formal RDA has been established because insufficient data exists to set a precise requirement. Importantly, the NIH ODS confirms no Tolerable Upper Limit for Vitamin K from food has been established — dietary Vitamin K is non-toxic. However, supplemental K1 interacts with warfarin.
Life Stage / Group | Adequate Intake — AI (µg/day) | Notes |
Infants 0–6 months | 2 µg (AI) | Neonates require IM prophylaxis — breast milk is very low in K1 |
Infants 7–12 months | 2.5 µg (AI) | |
Children 1–3 years | 30 µg | |
Children 4–8 years | 55 µg | |
Children 9–13 years | 60 µg | |
Teens 14–18 years | 75 µg | |
Men ≥19 years | 120 µg | No Tolerable Upper Limit established from food sources |
Women ≥19 years | 90 µg | No Tolerable Upper Limit from food. Supplemental K1 interacts with warfarin. |
Pregnant women | 90 µg | Avoid high-dose supplementation crosses placenta; neonatal risk if overdosed |
Lactating women | 90 µg | Breast milk K1 is low — neonatal IM prophylaxis remains essential regardless of maternal status |
Table 2. Vitamin K Adequate Intake (AI) by life stage. Source: NIH ODS
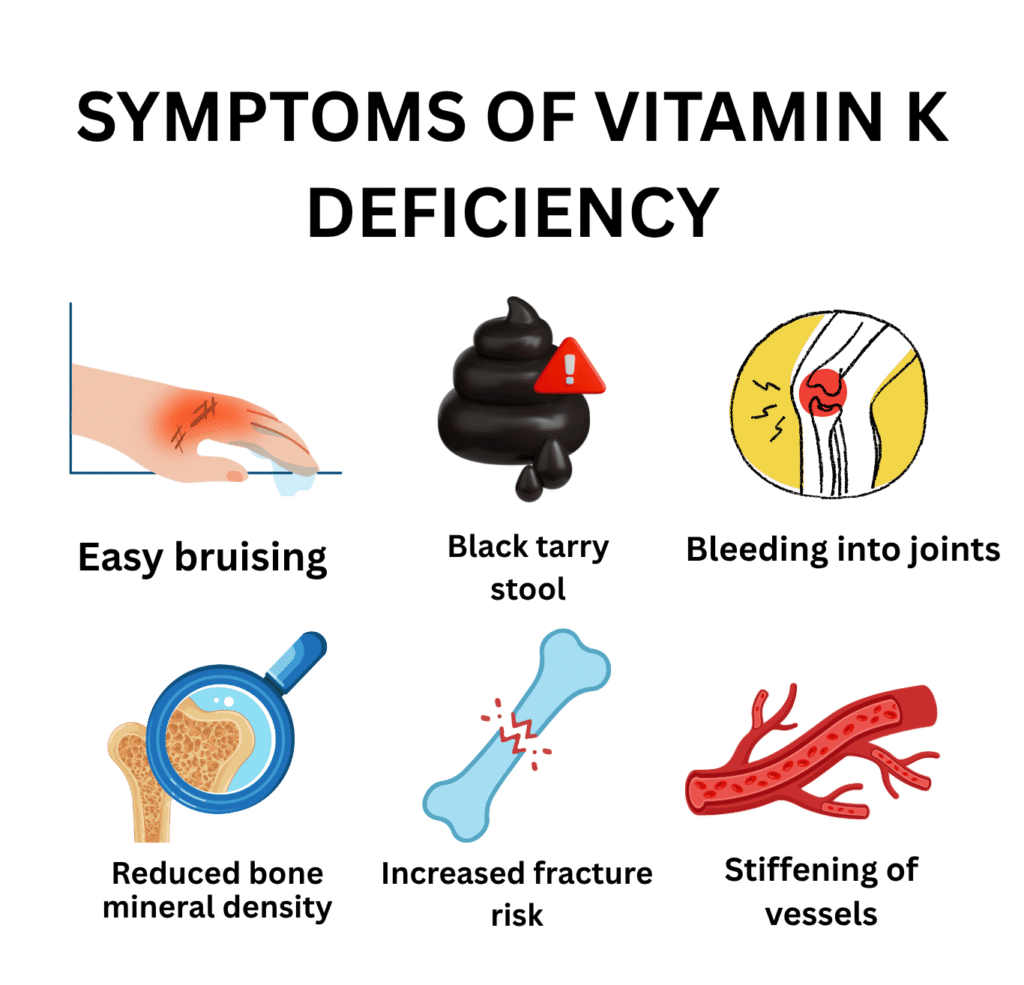
Vitamin K Deficiency Symptoms: Bleeding, Bruising, and the Bone and Heart Connection
The hallmark of Vitamin K deficiency is impaired haemostasis, the body’s inability to form and maintain a blood clot. Unlike platelet disorders (which cause superficial mucosal bleeding), Vitamin K deficiency causes deep tissue bleeding, large bruising, and haemorrhage at internal sites — similar to haemophilia.
System / Sign | Mild–Moderate Deficiency | Severe Deficiency |
Skin / External bleeding | Easy bruising; prolonged bleeding from minor cuts and wounds | Spontaneous large ecchymoses; haematomas from trivial trauma |
GI tract | Melaena (black tarry stool) — occult GI blood loss | Frank haematemesis (vomiting blood); severe GI haemorrhage |
Urinary tract | Microscopic haematuria | Macroscopic haematuria; haematoma around kidney |
Joints / Muscle | Haematomas after minor trauma | Haemarthrosis — bleeding into joints; large intramuscular haematomas |
Intracranial (neonates) | Irritability; bulging fontanelle | Intracranial haemorrhage — seizures, neurological devastation, death |
Bone (Vitamin K2 deficiency) | Reduced bone mineral density; increased fracture risk | Osteoporosis — particularly relevant in elderly and post-menopausal women |
Cardiovascular (K2 deficiency) | Arterial calcification — stiffening of vessels | Accelerated cardiovascular disease from uncontrolled vascular calcium deposition |
Menstrual | Heavy menstrual periods (menorrhagia) | Severe menorrhagia requiring transfusion |
Table 3. Vitamin K deficiency symptoms by severity and site. Sources: NCBI StatPearls; Merck Manual; CDC Jan 2025; PMC Ann Lab Med Jul 2025.
Key Symptoms in Clinical Detail
1. Easy Bruising and Prolonged Bleeding — The Cardinal Signs
Easy bruising from minor trauma and bleeding that takes far longer than normal to stop are the earliest clinical signs of Vitamin K deficiency. Patients describe:
- Large bruises from trivial bumps out of proportion to the injury
- Prolonged bleeding after cuts, dental procedures, or venepuncture
- Spontaneous bruising with no identifiable trauma
- Blood in urine or stool
The physical examination finding of ecchymoses and petechiae on the skin should always prompt measurement of PT/INR, the primary laboratory test of vitamin K-dependent coagulation.
2. Menorrhagia — Heavy Menstrual Bleeding
Heavy menstrual periods that are disproportionate and resistant to usual management can be a presenting symptom of Vitamin K deficiency, particularly in women with fat malabsorption conditions, those on anticonvulsants, or those on prolonged antibiotic courses. This connection is frequently overlooked in gynaecological practice.
3. The Bone and Cardiovascular Connection — Vitamin K2 Deficiency
The non-coagulation consequences of Vitamin K deficiency — particularly K2 — are less well-known but clinically significant:
- Osteoporosis: Vitamin K2 activates osteocalcin, which binds calcium into bone matrix. Deficiency leads to reduced bone mineralisation — contributing to osteoporosis independently of calcium and Vitamin D deficiency. A 2019 meta-analysis in Medicine found Vitamin K2 supplementation reduced fracture risk in osteoporotic patients.
- Arterial calcification: Matrix Gla Protein, activated by Vitamin K2, prevents calcium deposition in arterial walls. Deficiency allows uncontrolled vascular calcification, contributing to hypertension, arterial stiffness, and cardiovascular events. Low Vitamin K2 status is associated with increased coronary artery calcification scores in epidemiological studies.
💡 Clinical Insight: Any woman presenting with new-onset heavy menstrual bleeding should have a coagulation screen — PT, APTT, and platelet count — as part of the workup. Vitamin K deficiency is an underappreciated cause of menorrhagia.
VKDB: Vitamin K Deficiency Bleeding in Newborns
VKDB is the most acute and most preventable clinical manifestation of Vitamin K deficiency. Every newborn on earth is at risk — because neonates are born with:
- Virtually no gut bacteria to synthesise Vitamin K2
- Minimal hepatic Vitamin K stores — placental transfer of Vitamin K is limited
- Breast milk containing very low Vitamin K1 (1–4 µg/L) — far below the neonatal requirement
- Immature hepatic synthesis of coagulation factors
The result: without prophylaxis, the coagulation system of a newborn — particularly a breastfed newborn — is operating at critically low reserve.
VKDB Type | Timing | Clinical Features | Risk Without Prophylaxis |
Early VKDB | Within 24 hours of birth | Intracranial, intrathoracic, or intra-abdominal haemorrhage. Cephalhaematoma. Often severe and life-threatening. | 6–12% of at-risk newborns. Strongly linked to maternal medications — warfarin, anticonvulsants, antituberculous drugs. |
Classic VKDB | Days 2–7 of life | Bleeding from umbilical stump, circumcision site, skin bruising, GI bleeding (melaena). Most common form in healthy unsupplemented neonates. | 0.25–1.7 per 100 births without prophylaxis. Almost entirely preventable with IM vitamin K at birth. |
Late VKDB | Weeks 2–12 of life (up to 6 months) | Intracranial haemorrhage most common — often catastrophic. Associated with exclusively breastfed infants who did not receive vitamin K prophylaxis. | 4–7 per 100,000 without prophylaxis. Risk with IM vitamin K at birth: approximately 1 per 100,000. |
Table 4. VKDB classification by timing. Sources: PMC Ann Lab Med Jul 2025; Medscape Aug 2025; NCBI StatPearls; CDC Jan 2025
The Statistics That Make the Case for Prophylaxis Unanswerable
The Medscape review (August 2025) provides the definitive numbers:
- Without IM Vitamin K at birth: VKDB risk = 1,700 per 100,000 infants
- With IM Vitamin K at birth: VKDB risk = 1 per 100,000 infants
- A 1,700-fold reduction in risk from a single injection that costs pennies
- Late VKDB — the form causing intracranial haemorrhage — is almost entirely eliminated by birth prophylaxis
The CDC (January 2025) states explicitly: ‘In the majority of cases of VKDB, there are NO WARNING SIGNS before a life-threatening event starts.’ There is no early symptom stage that allows time to intervene. By the time VKDB is clinically apparent, intracranial haemorrhage has often already occurred
⚠️ Warning: Vitamin K prophylaxis at birth is not optional. Declining it places a healthy newborn at 1,700-fold increased risk of potentially fatal or brain-damaging haemorrhage — with no warning signs. There is no scientifically credible argument against it. Intramuscular phytomenadione 1 mg at birth is among the most beneficial interventions in all of medicine.
VKDB and Maternal Medications – The Foetal Risk
Certain maternal medications taken during pregnancy cross the placenta and inhibit foetal Vitamin K metabolism — causing early VKDB within 24 hours of birth. The PMC Ann Lab Med review (July 2025) identifies the key offenders:
- Warfarin and coumarin anticoagulants — directly block foetal VKOR enzyme
- Anticonvulsants — phenytoin, carbamazepine, phenobarbitone — accelerate Vitamin K catabolism
- Antituberculous drugs — isoniazid, rifampicin — impair Vitamin K metabolism
- Cephalosporin antibiotics — MTT side chain variants directly inhibit VKOR
💡 Clinical Insight: Any woman presenting with new-onset heavy menstrual bleeding should have a coagulation screen — PT, APTT, and platelet count — as part of the workup. Vitamin K deficiency is an underappreciated cause of menorrhagia.
The Warfarin-Vitamin K Relationship — Understanding Both Drugs
Warfarin is one of the world’s most widely prescribed anticoagulants — and understanding its mechanism requires understanding Vitamin K completely, because warfarin works entirely by blocking Vitamin K recycling.
How Warfarin Works
Warfarin inhibits Vitamin K epoxide reductase (VKOR) — the enzyme that recycles Vitamin K epoxide back to active Vitamin K. The result:
- Vitamin K is progressively depleted in the liver
- Vitamin K-dependent clotting factors (II, VII, IX, X) can no longer be carboxylated and activated
- Anticoagulant proteins C and S are also affected — but fall faster than procoagulant factors initially, creating a brief pro-thrombotic window when warfarin is first started
- INR rises as clotting time prolongs — the therapeutic target
Factors That Amplify Warfarin’s Effect — Drug Interactions
Any factor that reduces Vitamin K availability amplifies warfarin’s anticoagulant effect — potentially to dangerous levels:
- Antibiotics — especially fluoroquinolones and metronidazole: kill gut bacteria → reduce K2 synthesis → potentiate warfarin → INR rises sharply
- Dietary K1 reduction: patients who suddenly eat much less green leafy vegetables lose the dietary K1 that was partly offsetting warfarin’s effect → INR rises
- Liver disease: impairs activation of clotting factors regardless of Vitamin K status
- Many medications: amiodarone, fluconazole, NSAIDs, certain herbal supplements (St John’s Wort, ginkgo, garlic)
Warfarin Reversal — The Clinical Approach
Reversing excessive warfarin anticoagulation uses Vitamin K1 (phytomenadione) — which bypasses the blocked VKOR enzyme by providing fresh active Vitamin K directly. Speed of reversal depends on the route and urgency:
- Oral Vitamin K: 24–48 hours to normalise INR — appropriate for non-urgent supratherapeutic INR without bleeding
- IV Vitamin K: 4–6 hours — for significant bleeding or urgent reversal
- 4-factor PCC (prothrombin complex concentrate): 15–30 minutes — for life-threatening bleeding. Contains Factors II, VII, IX, X, Proteins C and S — provides immediate replacement of all depleted factors
- Fresh frozen plasma (FFP): contains all clotting factors — slower than PCC, requires large volumes
⚠️ Warning: When reversing warfarin for life-threatening bleeding — give 4-factor PCC immediately alongside IV Vitamin K. Do not wait for Vitamin K to work (4–6 hours) in a patient with intracranial haemorrhage. PCC is the drug that saves lives in this scenario. Vitamin K prevents re-anticoagulation over the following days.
What Causes Vitamin K Deficiency? Every Cause Explained
Cause | Specific Cause | Mechanism |
Drug — Vitamin K antagonist | Warfarin (coumadin), acenocoumarol, phenprocoumon | Directly inhibit Vitamin K epoxide reductase (VKOR) — the enzyme that recycles Vitamin K to its active form. This is the therapeutic mechanism. Excess dosing or interactions cause Vitamin K functional deficiency and bleeding. |
Drug — antibiotic effect | Broad-spectrum antibiotics (cephalosporins, fluoroquinolones, metronidazole) | Destroy gut bacteria that synthesise Vitamin K2. Particularly relevant in prolonged courses. Some cephalosporins (MTT side chain) also directly inhibit VKOR. |
Fat malabsorption | Coeliac disease, Crohn’s, cystic fibrosis, cholestatic liver disease, short bowel | Vitamin K is fat-soluble — absorption requires bile acids and micellar formation. Any fat malabsorption syndrome depletes all four fat-soluble vitamins simultaneously. |
Liver disease | Cirrhosis, severe hepatitis, liver failure | Even with adequate Vitamin K, the liver cannot synthesise clotting factors — Vitamin K supplementation does not fully correct the coagulopathy of liver failure. Both Vitamin K deficiency AND impaired synthesis coexist. |
Neonatal | All newborns — especially breastfed | Neonates are born with virtually no gut bacteria and have extremely low Vitamin K stores. Breast milk contains very little Vitamin K1 (1–4 µg/L vs formula 55 µg/L). Without prophylaxis, risk of VKDB is 1,700 per 100,000. |
Maternal medications | Maternal warfarin, anticonvulsants (phenytoin, carbamazepine), antituberculous drugs (isoniazid, rifampicin) | Cross the placenta and inhibit foetal and neonatal Vitamin K metabolism — causing early VKDB within 24 hours of birth. Affects 6–12% of exposed neonates. |
Dietary (rare) | Severely restricted diet very low in green vegetables | Pure dietary deficiency is extremely rare in adults — gut bacterial synthesis provides approximately half the daily requirement. Only in severely malnourished patients or those on parenteral nutrition without Vitamin K supplementation. |
Genetic | VKCFD — Vitamin K-dependent Clotting Factor Deficiency | Rare autosomal recessive mutations in GGCX (gamma-glutamyl carboxylase) or VKORC1 genes — enzymes essential for Vitamin K-dependent carboxylation. All Vitamin K-dependent factors and proteins are simultaneously deficient. |
Table 5. Complete causes of Vitamin K deficiency. Sources: NCBI StatPearls; Merck Manual; PMC Ann Lab Med Jul 2025; NIH ODS
How Is Vitamin K Deficiency Diagnosed?
Vitamin K deficiency is diagnosed through coagulation testing — not through a direct vitamin level measurement, which is not widely available in routine practice.
Primary Diagnostic Tests
- Prothrombin time (PT) and INR: the most sensitive and clinically relevant test. PT measures the time for plasma to clot via the extrinsic pathway — which requires Factors VII, X, V, II, and fibrinogen. Factor VII has the shortest half-life (4–6 hours) — its rapid depletion in Vitamin K deficiency makes PT the earliest abnormal test. INR = (patient PT / normal PT) raised to the power of the ISI.
- APTT (activated partial thromboplastin time): also prolonged in Vitamin K deficiency — reflecting deficiency of the intrinsic pathway factors (IX and X). Less sensitive than PT for early Vitamin K deficiency.
- PIVKA-II (Protein Induced by Vitamin K Absence or Antagonism — Factor II): the most sensitive functional marker of Vitamin K status. Measures uncarboxylated (inactive) prothrombin — which accumulates when Vitamin K is insufficient. PIVKA-II rises before PT prolongs — it is the earliest biochemical indicator of deficiency. Used for neonatal VKDB diagnosis and monitoring.
Supporting Tests
- Mixing study: mixing patient plasma with normal plasma corrects PT in factor deficiency (including Vitamin K deficiency) — but not in the presence of inhibitors (such as lupus anticoagulant). Useful to differentiate the cause of prolonged PT.
- Individual factor assays: Factors II, VII, IX, X — all low in Vitamin K deficiency; normal in von Willebrand disease
- Platelet count: normal in isolated Vitamin K deficiency — abnormal in DIC (disseminated intravascular coagulation), which can mimic Vitamin K deficiency
- Liver function tests: to assess hepatic contribution to coagulopathy
- Vitamin K therapeutic trial: if INR normalises within 24–48 hours of Vitamin K administration — Vitamin K deficiency was the cause. If it does not improve — liver synthetic failure is dominant
Vitamin K Deficiency Treatment: Phytomenadione, PCC, and the Prophylaxis Imperative
Treatment is with phytomenadione (Vitamin K1) — the synthetic form used in clinical medicine. The route, dose, and urgency depend entirely on the clinical scenario.
Clinical Scenario | Treatment | Rate / Duration / Notes |
VKDB — neonatal prophylaxis (standard) | IM phytomenadione (Vitamin K1) 1 mg at birth — single injection | Reduces VKDB risk from 1,700 to 1 per 100,000. Single most effective neonatal intervention. Safe; no adverse effects documented. |
VKDB — confirmed active bleeding in neonate | IV phytomenadione 0.3 mg/kg PLUS fresh frozen plasma (FFP) 10–20 ml/kg for immediate factor replacement | FFP provides immediate clotting factors. Vitamin K alone takes 4–6 hours to work — FFP bridges until synthesis is restored. |
Warfarin reversal — non-urgent (INR > 5, no bleeding) | Withhold warfarin. Oral phytomenadione 1–5 mg. | INR should fall within 24–48 hours. Restart warfarin at lower dose when INR in therapeutic range. |
Warfarin reversal — urgent (significant bleeding) | IV phytomenadione 5–10 mg over 20–60 minutes PLUS 4-factor PCC (prothrombin complex concentrate) or FFP | PCC (Beriplex, Octaplex) preferred over FFP for speed — provides all Vitamin K-dependent factors immediately. Vitamin K IV effect within 4–6 hours. |
Warfarin reversal — life-threatening bleeding (intracranial) | IV phytomenadione 10 mg PLUS 4-factor PCC immediately. Neurosurgical review. | Time-critical emergency. PCC reverses INR within 15–30 minutes. Do not wait for IV Vitamin K to work — give PCC simultaneously. |
Fat malabsorption-related deficiency | Water-miscible phytomenadione orally OR IM/SC injection. Dose guided by INR and PIVKA-II. | Standard fat-soluble supplements poorly absorbed. Treat underlying malabsorption condition alongside. |
Dietary / antibiotic-induced deficiency | Oral phytomenadione 5–10 mg/day until coagulopathy corrects | INR should normalise within 2–3 days. Ensure dietary Vitamin K intake is adequate ongoing. |
Liver disease coagulopathy | Oral or IV phytomenadione 10 mg/day for 3 days — trial of supplementation. If INR improves, Vitamin K deficiency was contributing. | If INR does not improve after 3 days of Vitamin K — liver synthetic failure is the dominant cause, not vitamin deficiency. FFP for bleeding episodes. |
Table 6. Vitamin K deficiency treatment protocol. Sources: NCBI StatPearls; PMC Ann Lab Med Jul 2025; Merck Manual; NHS guidelines.
Recovery Timeline
What Improves | Timeline After Treatment |
INR normalisation — oral Vitamin K | 24–48 hours |
INR normalisation — IV Vitamin K | 4–6 hours |
INR normalisation — 4-factor PCC | 15–30 minutes |
Bleeding cessation | Hours after clotting factors activated |
VKDB — intracranial haemorrhage neurological recovery | Variable — depends on severity and speed of treatment. Some deficits permanent. |
Bone density (K2 deficiency, long-term) | 12–24 months of adequate K2 alongside calcium and Vitamin D |
Table 7. Recovery timeline after Vitamin K treatment. Source: Clinical experience + Merck Manual; NCBI StatPearls; PMC Ann Lab Med Jul 2025.
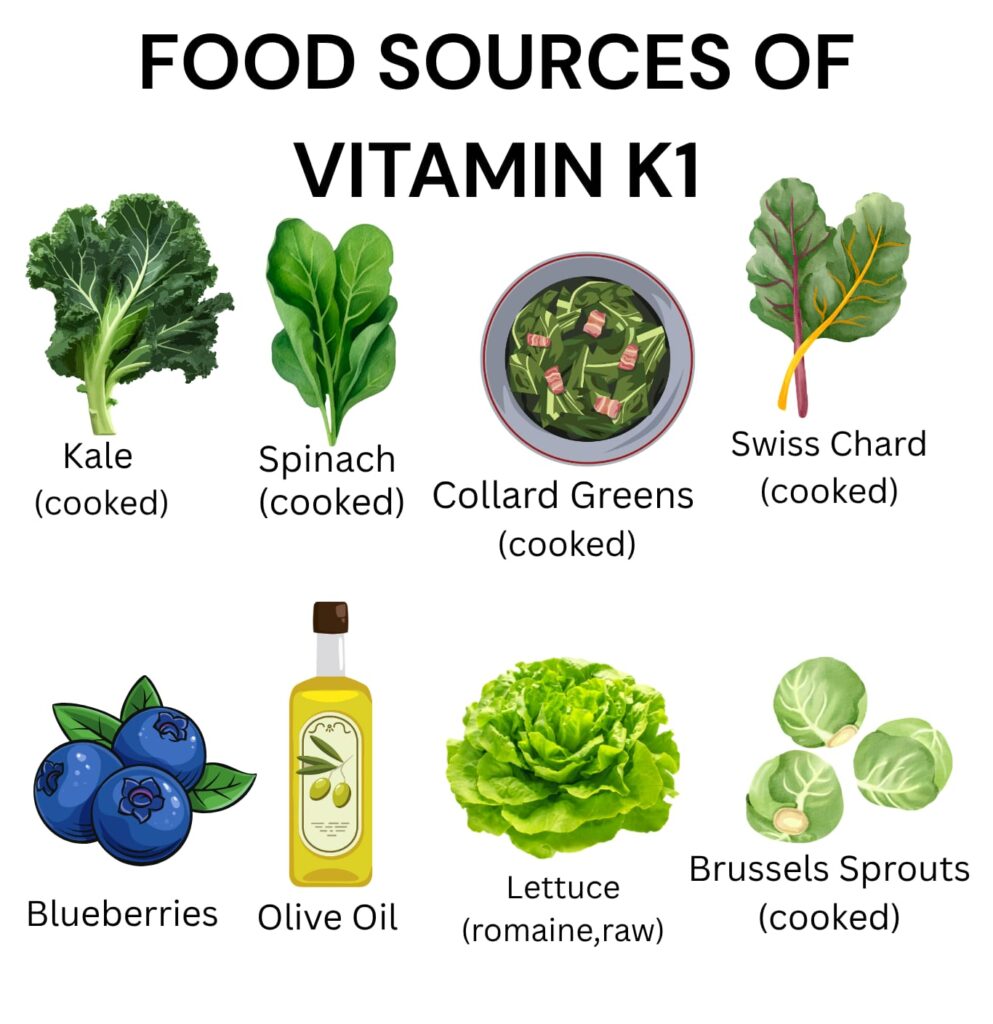
Best Food Sources of Vitamin K
Vitamin K1 is found almost exclusively in dark green leafy vegetables and plant oils. Vitamin K2 is found in fermented foods, certain cheeses, and animal products. For adequate intake of both forms, dietary diversity matters more than any single food.
System | Serving | Vitamin K (µg) | Type |
Natto (fermented soya beans) | 85 g (3 oz) | 850 µg ✦ Highest K2 | K2 (MK-7) — highest K2 food |
Kale (raw) | 1 cup (~67 g) | 472 µg | K1 (phylloquinone) |
Collard greens (cooked) | ½ cup (~95 g) | 530 µg | K1 |
Spinach (raw) | 1 cup (~30 g) | 145 µg | K1 |
Broccoli (cooked) | ½ cup (~78 g) | 110 µg | K1 |
Brussels sprouts (cooked) | ½ cup (~78 g) | 109 µg | K1 |
Soybean oil | 1 tablespoon (14 ml) | 25 µg | K1 |
Canola oil | 1 tablespoon (14 ml) | 17 µg | K1 |
Cheese (hard, e.g. Gouda) | 28 g (1 oz) | 10–75 µg | K2 (MK-4 to MK-9) |
Egg yolk | 1 large | 4 µg | K2 (MK-4) |
Table 8. Top dietary sources of Vitamin K (K1 and K2). Source: NIH ODS / USDA FoodData Central. Adult men AI = 120 µg/day; women = 90 µg/day.
⚠️ The Warfarin-Diet Interaction: Patients on warfarin are often told to ‘avoid green vegetables’ — this is incorrect advice. The correct instruction is to keep vitamin K intake CONSISTENT, not to restrict it. Sudden large increases in green vegetable intake lower INR; sudden reductions raise it. A consistent moderate intake is what maintains stable anticoagulation. Eliminating K1-rich vegetables deprives patients of essential nutrients unnecessarily.
How to Prevent Vitamin K Deficiency
The Non-Negotiable Prevention — Neonatal IM Prophylaxis
- Single IM phytomenadione 1 mg at birth — for every newborn, regardless of feeding method, health status, or gestational age
- Reduces late VKDB risk from 4–7 per 100,000 to essentially zero
- Safe — no documented adverse effects from IM Vitamin K prophylaxis
- The ‘link’ to childhood leukaemia proposed in the 1990s has been definitively refuted by multiple large studies
- Oral prophylaxis regimens exist but are inferior to IM — particularly for late VKDB prevention
For the General Population
- Eat dark green leafy vegetables daily — kale, spinach, broccoli, Brussels sprouts
- Include fermented foods for K2 — cheese, yoghurt, natto where available
- Use plant oils — soybean and canola oil in cooking contribute meaningful K1
For High-Risk Groups
- Patients on warfarin: consistent dietary K1 intake — not restriction; regular INR monitoring; counselling about antibiotic interactions
- Fat malabsorption conditions: annual fat-soluble vitamin monitoring including Vitamin K (PT/INR, PIVKA-II); water-miscible supplementation if deficient
- Patients on long-term antibiotics: Vitamin K monitoring, especially if on warfarin simultaneously
- Patients on anticonvulsants: annual Vitamin K status monitoring; supplementation if PT is prolonged
- Liver disease patients: regular coagulation monitoring; empirical Vitamin K trial before ascribing all coagulopathy to liver failure
Vitamin K vs Vitamin E vs Vitamin A — How to Tell Them Apart
Feature | Vitamin K Deficiency | Vitamin E Deficiency | Vitamin A Deficiency |
Primary manifestation | Abnormal bleeding and bruising | Spinocerebellar ataxia; neuropathy | Night blindness; keratomalacia |
Neonatal emergency? | Yes — VKDB; intracranial haemorrhage | Yes — haemolytic anaemia in premature infants | Yes — infantile blindness |
Key diagnostic test | PT/INR; PIVKA-II | Serum alpha-tocopherol / lipid ratio | Serum retinol |
Drug interaction? | Yes — warfarin antagonism is fundamental | Yes — high-dose Vitamin E affects clotting | Yes — teratogenic at high doses |
Beyond clotting / vision? | Yes — bone mineralisation; arterial calcification prevention | Antioxidant protection of all membranes | Immune function; epithelial integrity |
Prevention of neonatal form | Single IM injection at birth | NICU supplementation protocol | Maternal supplementation; fortification |
Table 9. Comparative guide — Vitamin K vs E vs A deficiency. Source: Clinical experience + NIH ODS; NCBI StatPearls; Merck Manual.
Frequently Asked Questions About Vitamin K Deficiency
RELATED ARTICLES
- Nutritional Deficiency Diseases: The Complete Guide
- Vitamin D Deficiency: Symptoms, Causes and Treatment
- Calcium Deficiency and Hypocalcaemia: The Complete Guide
- Iron Deficiency and Anaemia: Symptoms and Treatment
- Folate Deficiency: Folic Acid, Pregnancy and Prevention
- Vitamin B12 Deficiency: Nerves, Anaemia and Treatment
- Vitamin A Deficiency: Night Blindness and Prevention
- Magnesium Deficiency: Symptoms and Best Supplement Forms
- Zinc Deficiency: Immunity, Hair Loss and Treatment
- Vitamin C Deficiency and Scurvy: The Complete Guide
- Iodine Deficiency: Goitre, Hypothyroidism and Treatment
REFERENCES
- NIH Office of Dietary Supplements. Vitamin K Fact Sheet for Health Professionals. Updated 2024.
- NCBI StatPearls. Vitamin K Deficiency. 2025.
- Merck Manual Professional Edition. Vitamin K Deficiency.
- Shearer MJ, Fu X, Booth SL. Vitamin K nutrition, metabolism, and requirements: current concepts and future research. Adv Nutr. 2012;3(2):182-195.
- Brinkman HJM, Schurgers L, et al. Vitamin K2 supplementation and arterial stiffness. Thromb Haemost. 2015.
- van Ballegooijen AJ, Pilz S, Tomaschitz A, et al. The synergistic interplay between vitamins D and K for bone and cardiovascular health: a narrative review. Int J Endocrinol. 2017.
- Mihatsch WA, et al. Prevention of Vitamin K Deficiency Bleeding in Newborn Infants. Ann Nutr Metab. 2016;68(Suppl 3):1-7.
- Cleveland Clinic. Vitamin K Deficiency.
- British Dietetic Association. Vitamin K Food Fact Sheet.
- Fusaro M, et al. Vitamin K2 and bone mineral density in the elderly. J Bone Miner Res. 2020.
DISCLAIMER
MEDICAL DISCLAIMER: This article is written for educational purposes by a qualified physician. It does not constitute personal medical advice. If you are on warfarin or any anticoagulant, do not change your diet or start any supplement without discussing it with your prescribing physician first. Individual symptoms, test results, and treatment decisions must be discussed with a qualified healthcare provider. Never self-diagnose or self-treat bleeding disorders on the basis of any article, including this one.