
Zinc Deficiency: Symptoms, Causes, Diagnosis, Treatment and Prevention – The Complete Doctor’s Guide
The mineral behind immunity, taste, wound healing, and your child’s growth. Why 2 billion people do not get enough.
✍️ Written and reviewed by: Prof. Dr Qazi Taqweemulhaq, FCPS Medicine — Professor of Medicine, Women Medical and Dental College, Abbottabad, Pakistan. Consultant Physician, 32 Years Clinical Experience
📅 Last Updated: May 2026 | References: WHO, NIH ODS, NCBI StatPearls (Aug 2025), Nature Scientific Reports 2024, IFPRI 2024, Cleveland Clinic, Merck Manual
⚡ Quick Answer: Zinc deficiency affects an estimated 17 to 31% of the global population, over 2 billion people. It causes loss of taste and smell, impaired immunity, slow wound healing, hair loss, growth stunting in children, and skin problems. Serum zinc is unreliable — normal levels can coexist with significant cellular depletion. Treatment is elemental zinc 25 to 40 mg per day orally. Do not exceed 40 mg per day chronically. High-dose zinc depletes copper and causes copper-deficiency anaemia and neuropathy.
|
✅ KEY TAKEAWAYS — Zinc Deficiency |
|
Zinc deficiency affects an estimated 17 to 31% of the global population, more than 2 billion people |
|
• Loss of taste (dysgeusia) and loss of smell (anosmia) are hallmark symptoms and highly specific to zinc deficiency |
|
• Zinc is essential for immunity. Deficiency dramatically increases susceptibility to pneumonia, diarrhoea, and malaria in children |
|
• Serum zinc is unreliable. It can appear normal even with significant cellular deficiency. Clinical picture must guide management |
|
• Excess zinc supplementation above 40 mg per day chronically depletes copper, causing copper-deficiency anaemia and neuropathy |
|
• Acrodermatitis enteropathica is a genetic form of zinc deficiency. It is a medical emergency in infants with a classic triad of perioral dermatitis, diarrhoea, and alopecia |
The Mineral Behind Your Taste,Your Immunity, and Your Body’s Ability to Heal Itself
There is one question I ask every patient with unexplained fatigue, recurrent infections, poor wound healing, or significant hair loss.
Has your sense of taste or smell changed recently?
The answer is yes more often than most clinicians would expect. Food no longer tastes right. Favourite dishes smell wrong. Coffee has lost its aroma. These are not vague complaints. They are specific, diagnostically useful symptoms pointing directly to zinc deficiency, a condition affecting more than 2 billion people worldwide that receives far less clinical attention than it deserves.
Zinc deficiency is one of the ten most significant contributors to disease burden in the developing world, according to the WHO. Yet it is investigated last, if at all, in most clinical workups. Patients spend months being tested for thyroid disease, anaemia, and depression before anyone checks their zinc.
In children, low zinc causes stunting, immune failure, and increased death from pneumonia, diarrhoea, and malaria. In adults, it causes impaired wound healing, recurrent infections, hair loss, and reproductive dysfunction.
In the elderly, a 2025 PMC review from RWTH Aachen University estimated that up to 75% of individuals aged 65 to 84 have inadequate zinc intake. That figure accelerates immune ageing and contributes meaningfully to cardiovascular disease and diabetes in this population.
Every immune cell requires zinc. Every wound that heals requires it. Every time you taste food or smell something, you depend on it. Roughly one in five people reading this article is not getting enough
⚡ Quick Answer: During the COVID-19 pandemic I saw many patients with persistent loss of taste and smell weeks or months after recovering from infection. When I checked zinc levels in those with the most prolonged symptoms, a significant proportion were deficient. Zinc is required for the repair of chemosensory receptor cells. Correcting zinc deficiency in these patients accelerated recovery of taste and smell.
What Is Zinc and What Does It Do?
Zinc is an essential trace mineral. It is the second most abundant trace element in the human body after iron. Total body zinc is approximately 2 to 3 grams, distributed across muscle (60%), bone (30%), and the liver, skin, kidney, and other tissues (10%).
Serum zinc is less than 0.1% of total body zinc. That single fact explains why serum zinc is such a poor marker of total body stores.
Unlike iron, the body has no dedicated zinc storage system. Skeletal muscle zinc is tightly bound and not readily mobilised. The body depends heavily on daily dietary zinc intake. A short period of inadequate intake depletes functional zinc pools relatively quickly.
The Ten Critical Functions of Zinc
- Immune function. Zinc is required for the development and activation of virtually all immune cells. T and B lymphocytes, natural killer cells, macrophages, and neutrophils all need it. Zinc regulates inflammatory cytokine production, maintains thymic function, and activates thymulin, a thymic hormone essential for T-cell maturation. Zinc deficiency produces a state of immunodeficiency that is both cellular and humoral.
- Wound healing. Zinc is required at every phase of wound repair. Haemostasis, inflammation, fibroblast proliferation, and collagen synthesis all depend on it. Zinc activates matrix metalloproteinases needed for tissue remodelling. Zinc-deficient wounds heal slowly, incompletely, or not at all.
- Taste and smell. Zinc is a structural component of gustin, also known as carbonic anhydrase VI, a salivary protein essential for taste receptor function. It is also required for normal olfactory receptor maintenance. Loss of taste and loss of smell are among the most specific clinical symptoms of zinc deficiency.
- Protein synthesis and cell division. Zinc is a cofactor for over 300 enzymes and over 1,000 transcription factors involved in DNA synthesis, RNA transcription, and protein production. Every dividing cell requires it.
- Growth and development. Zinc is required for growth hormone synthesis and action, IGF-1 production, and the proliferation of growth plate cells. Deficiency causes stunting in children, low height for age, one of the most visible and lasting consequences.
- Antioxidant defence. Zinc is a structural component of copper-zinc superoxide dismutase (CuZnSOD), one of the body’s most important antioxidant enzymes. It also stabilises cell membranes against oxidative damage.
- Reproductive function. Zinc is highly concentrated in the testes and essential for testosterone synthesis, sperm production, and sperm motility. In females, it regulates ovarian follicle development and ovulation.
- Vision. Zinc is found in high concentrations in the retina and choroid. It is required for the conversion of retinol to retinal, the visual pigment. Deficiency can impair night vision and may accelerate age-related macular degeneration.
- Insulin storage and release. Zinc is required for the crystallisation and storage of insulin in pancreatic beta cells and for its release in response to glucose. Deficiency impairs glucose metabolism and may worsen insulin resistance.
- Gene expression. Zinc finger proteins, transcription factors with zinc at their core, regulate the expression of thousands of genes controlling immune function, growth, and cancer suppression.
How Much Zinc Do You Need Per Day?
The upper tolerable intake level of 40 mg per day applies to total zinc from all sources. Exceeding this chronically depletes copper. This is a serious risk that most people taking zinc supplements are never warned about. See the toxicity section below.
|
Life Stage / Group |
RDA (mg/day) |
Upper Limit (mg/day) |
|
Infants 0–6 months |
2 mg |
4 mg |
|
Children 1–3 years |
3 mg |
7 mg |
|
Children 4–8 years |
5 mg |
12 mg |
|
Children 9–13 years |
8 mg |
23 mg |
|
Teen boys 14–18 years |
11 mg |
34 mg |
|
Teen girls 14–18 years |
9 mg |
34 mg |
|
Men ≥19 years |
11 mg |
40 mg |
|
Women ≥19 years |
8 mg |
40 mg |
|
Pregnant women |
11 mg |
40 mg |
|
Breastfeeding women |
12 mg |
40 mg |
Table 1. Zinc RDA and Tolerable Upper Intake Levels. Source: NIH ODS; NCBI StatPearls (Updated August 2025).
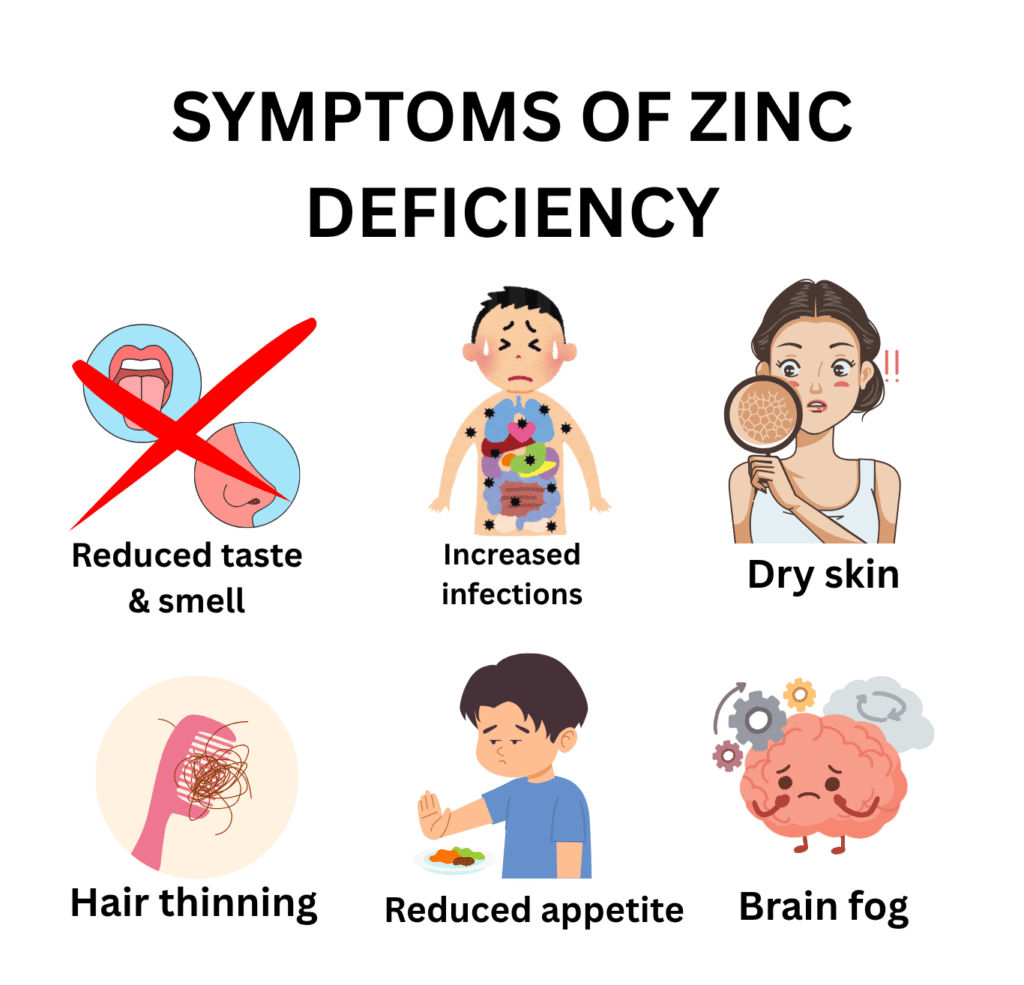
Zinc Deficiency Symptoms: What Your Body Is Telling You
Zinc deficiency is sometimes called the great imitator. Its symptoms overlap with many other conditions and are easily attributed to ageing, stress, or other diagnoses. Loss of taste and smell is the most diagnostically specific symptom. Any patient who reports a change in taste or smell should have a zinc level checked.
|
System |
Mild–Moderate Deficiency |
Severe / Prolonged Deficiency |
|
Taste and Smell |
Reduced taste (dysgeusia) and smell (hyposmia) often first noticed |
Complete loss of taste (ageusia) and smell (anosmia) |
|
Immunity |
Increased frequency of infections; slow recovery |
Severely impaired immunity, recurrent pneumonia, diarrhoea, skin infections |
|
Skin |
Dry skin, slow wound healing, acne-like eruptions |
Dermatitis, perioral, perianal, and acral; alopecia; severe wound non-healing |
|
Hair |
Hair thinning and increased shedding |
Diffuse alopecia, significant hair loss |
|
Growth (children) |
Reduced appetite, mild growth slowing |
Stunting, low height for age; hypogonadism in adolescent boys |
|
Eyes |
Reduced night vision (zinc needed for retinal rhodopsin) |
Photophobia; corneal clouding particularly in severe deficiency |
|
Neurological |
Brain fog, irritability, depression |
Cognitive impairment; delayed neurological development in children |
|
Reproductive |
Reduced libido; impaired sperm quality |
Hypogonadism in males; delayed sexual maturation; infertility |
|
GI |
Reduced appetite, nausea |
Diarrhoea, both a cause and consequence of zinc deficiency |
Table 2. Zinc deficiency symptoms by severity and organ system. Sources: NCBI StatPearls (Aug 2025); NIH ODS; Cleveland Clinic; Merck Manual.
The Symptoms in Clinical Detail
1. Loss of Taste and Smell, The Most Specific Symptom
Patients with zinc deficiency describe food that previously tasted rich now seeming bland or tasteless, metallic or distorted taste perception, favourite foods becoming unappealing, and an inability to detect familiar odours. These symptoms are highly specific. When a patient reports all of them together, zinc is the most likely explanation.
💡 Clinical Insight: During the COVID-19 pandemic, zinc deficiency was identified as a risk factor for the persistence of taste and smell loss in long COVID. Zinc is required for the repair of chemosensory receptor cells. Supplementation in deficient patients accelerated recovery in a way that time alone did not.
2. Impaired Wound Healing
Zinc-deficient wounds have:
- Reduced collagen synthesis, the structural framework of healing tissue
- Impaired fibroblast proliferation
- Reduced epithelialisation skin fails to close over the wound
- Increased susceptibility to wound infection
Clinically, this presents as wounds that heal slowly, incompletely, or repeatedly break down. In surgical patients, unrecognised zinc deficiency is a significant cause of poor postoperative healing.
3. Hair Loss and Skin Changes
Zinc deficiency causes:
- Diffuse alopecia: hair thins and sheds across the entire scalp, not patchy like alopecia areata
- Acneiform eruptions: zinc is anti-inflammatory and required for sebum regulation – deficiency worsens acne
- Perioral and perianal dermatitis: especially in severe deficiency, a classic pattern that should prompt immediate zinc testing
💡 Clinical Insight: Zinc is one of the most important nutritional supplements in dermatology. Low-dose oral zinc sulphate is used as a therapeutic option for acne vulgaris, with evidence comparable to some topical antibiotics.
4. Immune Failure and Recurrent Infections
Zinc deficiency produces a state of acquired immunodeficiency:
- Thymus atrophy → reduced T-cell production and maturation
- Impaired natural killer cell activity → reduced viral surveillance
- Reduced neutrophil bactericidal function
- Increased susceptibility to pneumonia, diarrhoea, and skin infections
In children, zinc supplementation reduces:
- Diarrhoeal disease duration by 25% and severity by 40% (WHO recommendation)
- Pneumonia incidence by approximately 41% in deficient children
- All-cause child mortality in zinc-supplemented populations
5. Growth Stunting in Children
Stunting, low height for age, is one of the most visible and lasting consequences of zinc deficiency. Zinc is required for:
- Growth hormone synthesis and IGF-1 production
- Proliferation of growth plate chondrocytes
- Normal appetite regulation. Zinc-deficient children eat less.
Zinc supplementation in deficient children produces measurable catch-up growth. The effect is most pronounced when supplementation begins in the first two years of life, the critical window for irreversible stunting.
Acrodermatitis Enteropathica (AE): The Genetic Form of Zinc Deficiency
Acrodermatitis enteropathica (AE) is a rare autosomal recessive genetic disorder caused by mutations in the SLC39A4 gene — which encodes ZIP4, the primary intestinal zinc transporter. Without functional ZIP4, dietary zinc cannot be absorbed from the gut, regardless of intake.
It is a medical emergency in infants — typically presenting when breastfeeding stops (breast milk contains a zinc-binding ligand that provides some absorption even without ZIP4). Classic presentation:
- Characteristic dermatitis: perioral (around the mouth), perianal, and acral (hands, feet, genitalia): often vesiculobullous, eczematous, or psoriasiform
- Diarrhoea: profuse and difficult to control
- Alopecia: total scalp hair loss
- Irritability and growth failure
- Secondary infections: Candida and bacterial superinfection of skin lesions
Treatment is lifelong oral zinc supplementation at 3 mg/kg/day elemental zinc. Symptoms resolve dramatically within days of starting treatment, one of the most gratifying responses in nutritional medicine. Without treatment, Acrodermatitis Enteropathica is fatal.
⚠️ Warning: Any infant presenting with the triad of perioral/perianal/acral dermatitis + diarrhoea + alopecia must have a serum zinc measured immediately. Acrodermatitis enteropathica is life-threatening without treatment and treatable with a simple, cheap supplement.
What Causes Zinc Deficiency? Every Cause Explained
|
Cause |
Specific Cause |
Key Mechanism |
|
Dietary |
Low meat / seafood diet : vegetarian, vegan |
Haem-containing foods (meat, shellfish) provide highly bioavailable zinc. Plant foods contain phytates that bind zinc and reduce absorption to 15–25% vs 40–50% from animal foods |
|
Phytate inhibition |
High phytate diet : whole grains, legumes, seeds |
Phytic acid (inositol hexaphosphate) chelates zinc in the gut, the primary dietary cause of zinc deficiency in populations eating predominantly plant-based staple diets. |
|
Malabsorption |
IBD (Crohn’s, UC), coeliac disease, short bowel |
Intestinal inflammation and reduced absorptive surface impair zinc uptake. IBD is a major cause, a recent 2025 study (King Faisal Specialist Hospital) found significant zinc deficiency rates in IBD patients |
|
Genetic |
Acrodermatitis enteropathica |
Autosomal recessive mutation in SLC39A4 gene, encodes the intestinal zinc transporter ZIP4. Severe zinc malabsorption from birth. Medical emergency in infants |
|
Alcohol |
Heavy or chronic alcohol consumption |
Alcohol reduces intestinal zinc absorption and increases urinary zinc excretion. Alcoholic liver disease further impairs zinc metabolism |
|
Increased demand |
Pregnancy, lactation, rapid childhood growth |
Zinc is required for foetal development, breast milk production, and cell division during growth. Demand exceeds dietary supply without supplementation in many cases |
|
Chronic diarrhoea |
Any cause of persistent diarrhoea |
Both a cause and a consequence of zinc deficiency, a vicious cycle. Zinc supplementation reduces diarrhoeal disease duration and severity in children |
|
Drug-induced |
Loop diuretics, ACE inhibitors, thiazides |
Diuretics increase urinary zinc excretion. Long-term use without monitoring can deplete zinc stores |
|
Excess zinc supplementation → copper depletion |
Taking > 40 mg/day zinc chronically |
Zinc and copper compete for intestinal absorption via metallothionein. High zinc induces metallothionein in gut cells, which traps copper and prevents its absorption. Causes copper-deficiency anaemia and neuropathy |
|
Ageing |
Adults over 65 years |
Reduced dietary intake, impaired absorption, medications. PMC 2025 review: up to 75% of individuals aged 65–84 may have inadequate zinc intake by EFSA guidelines |
Table 3. Complete causes of zinc deficiency. Sources: NCBI StatPearls (Aug 2025); NIH ODS; IFPRI 2024; Cleveland Clinic.
The Phytate Problem: Why Plant-Based Diets Increase Risk
Phytic acid (inositol hexaphosphate) is found in all whole grains, legumes, nuts, and seeds: exactly the foods that are highest in plant-based zinc. Phytic acid chelates zinc in the gut, forming insoluble zinc-phytate complexes that cannot be absorbed. The result:
- Zinc absorption from plant foods: 15–25%
- Zinc absorption from animal foods: 40–50%
- A vegetarian diet requires approximately 50% more dietary zinc than an omnivorous diet to achieve equivalent absorption
Practical strategies to reduce phytate inhibition:
- Soaking: soaking legumes and grains in water for 8–12 hours before cooking reduces phytate content by 30–50%
- Sprouting: germinating seeds activates phytase enzymes that break down phytic acid
- Fermentation: sourdough bread fermentation reduces phytate significantly compared to regular bread
- Eating Vitamin C with plant zinc sources: less potent for zinc than for iron, but some enhancement occurs
💡 Clinical Insight: Vegetarians and vegans need to actively plan their zinc intake, not just eat more legumes and whole grains. Without phytate-reduction techniques, the higher nominal zinc content of plant foods is misleading. Annual serum zinc monitoring is reasonable for anyone on a strictly plant-based diet.
How Is Zinc Deficiency Diagnosed?
Zinc deficiency is one of the most difficult nutritional deficiencies to diagnose accurately. This is because no single blood test reliably reflects total body zinc status. This is acknowledged in the medical literature and requires a clinical approach.
The Limitations of Serum Zinc
- Serum zinc represents < 0.1% of total body zinc, it is homeostically maintained and may appear normal despite significant cellular depletion
- Serum zinc falls in acute infection, inflammation, and stress making interpretation during illness unreliable
- Serum zinc rises after meals, results should be obtained fasting in the morning for consistency
- A borderline-low serum zinc in a symptomatic patient with risk factors is clinically significant, do not dismiss it based on marginal numbers
Interpretation of Serum Zinc
- Deficient: < 70 µg/dL (< 10.7 µmol/L) in adults fasting morning sample
- Marginal deficiency: 70–80 µg/dL : treat if symptomatic with risk factors
- Normal: > 80 µg/dL : but does not exclude cellular zinc depletion
Supporting Assessments
- 24-hour urinary zinc: low urinary zinc suggests conservation in response to deficiency
- Alkaline phosphatase (ALP) a zinc-dependent enzyme: levels fall in zinc deficiency. Rising ALP after supplementation confirms zinc-dependent enzyme restoration.
- Therapeutic trial: in patients with classic symptoms and risk factors, a 4–8 week trial of zinc supplementation is clinically justified even with borderline serum levels. Symptom response (particularly taste/smell improvement) confirms the diagnosis
- Full blood count and copper: to detect concurrent copper deficiency (especially in those previously on high-dose zinc)
💡 Clinical Insight: The most practical diagnostic approach: a patient with unexplained taste/smell loss, hair thinning, recurrent infections, slow wound healing, or a recognised risk factor (vegetarian diet, IBD, bariatric surgery, elderly age) should have serum zinc checked. If borderline, should receive a supervised therapeutic trial.
The clinical response to supplementation is itself diagnostic.
Zinc Deficiency Treatment: Which Form, How Much, and How Long?
All oral zinc salt forms: zinc sulphate, zinc gluconate, zinc acetate, zinc citrate are effective for treating deficiency.
Doses are expressed as elemental zinc. Always check the supplement label for elemental zinc content, as zinc salt doses are higher than elemental doses.
|
Clinical Scenario |
Treatment |
Duration & Notes |
|
Mild dietary zinc deficiency |
Elemental zinc 25–40 mg/day orally. Zinc sulphate, gluconate, or acetate all are effective |
4–8 weeks. Recheck serum zinc and symptoms. Correct dietary intake long-term |
|
Moderate to severe deficiency |
Elemental zinc 40–60 mg/day in divided doses |
Continue until symptoms resolve and serum zinc normalises. Consider copper monitoring if using high doses |
|
Acrodermatitis enteropathica |
Elemental zinc 3 mg/kg/day – lifelong supplementation |
Symptoms resolve within days. Lifelong therapy required. The genetic transport defect does not resolve. Monitor zinc levels annually |
|
Childhood diarrhoea (WHO protocol) |
Elemental zinc 20 mg/day for children > 6 months; 10 mg/day for infants 2–6 months × 10–14 days |
WHO recommendation for diarrhoea treatment in low-income settings. Reduces duration by 25% and severity by 40%. |
|
Post-bariatric surgery |
Zinc supplement as part of multivitamin-mineral protocol |
Lifelong supplementation. Annual zinc monitoring mandatory |
|
IBD (Crohn’s, UC) |
Oral zinc 25–40 mg elemental/day. Higher doses if malabsorption is severe |
Monitor both zinc and copper. Treat underlying IBD. Absorption will not normalise until gut inflammation is controlled |
|
Common cold (within 24 hrs of onset) |
Zinc acetate or gluconate lozenges 75–100 mg elemental zinc/day |
Evidence suggests 1–2 day reduction in cold duration when started within 24 hours of symptom onset. Short-course use only |
Table 4. Zinc deficiency treatment protocol. Sources: NCBI StatPearls (Aug 2025); WHO; NIH ODS; Cleveland Clinic.
Recovery Timeline
|
Patient Group |
Acute Treatment |
|
Taste and smell |
Days to 1–2 weeks : often the most gratifying early response |
|
Wound healing and skin |
2–4 weeks |
|
Hair loss stabilises |
4–8 weeks; hair regrowth over 3–6 months |
|
Immunity and infection frequency |
4–8 weeks of restored zinc status |
|
Growth (in children) |
Months of adequate zinc with overall nutritional improvement |
Table 5. Zinc deficiency recovery timeline. Source: Clinical experience + NCBI StatPearls.
Practical Supplementation Tips
- Take on an empty stomach: zinc absorption is approximately 40% better without food
- Avoid taking with calcium or iron: these minerals compete with zinc for absorption, separate by 2 hours
- Avoid taking with tea or coffee: tannins reduce zinc absorption
- Take with small amount of food if GI upset occurs: zinc sulphate is more likely to cause nausea than zinc gluconate or citrate, switch formulation if needed
- Monitor copper if using > 25 mg/day for more than 4 weeks: check serum copper and caeruloplasmin, the zinc-copper interaction is dose-dependent and time-dependent
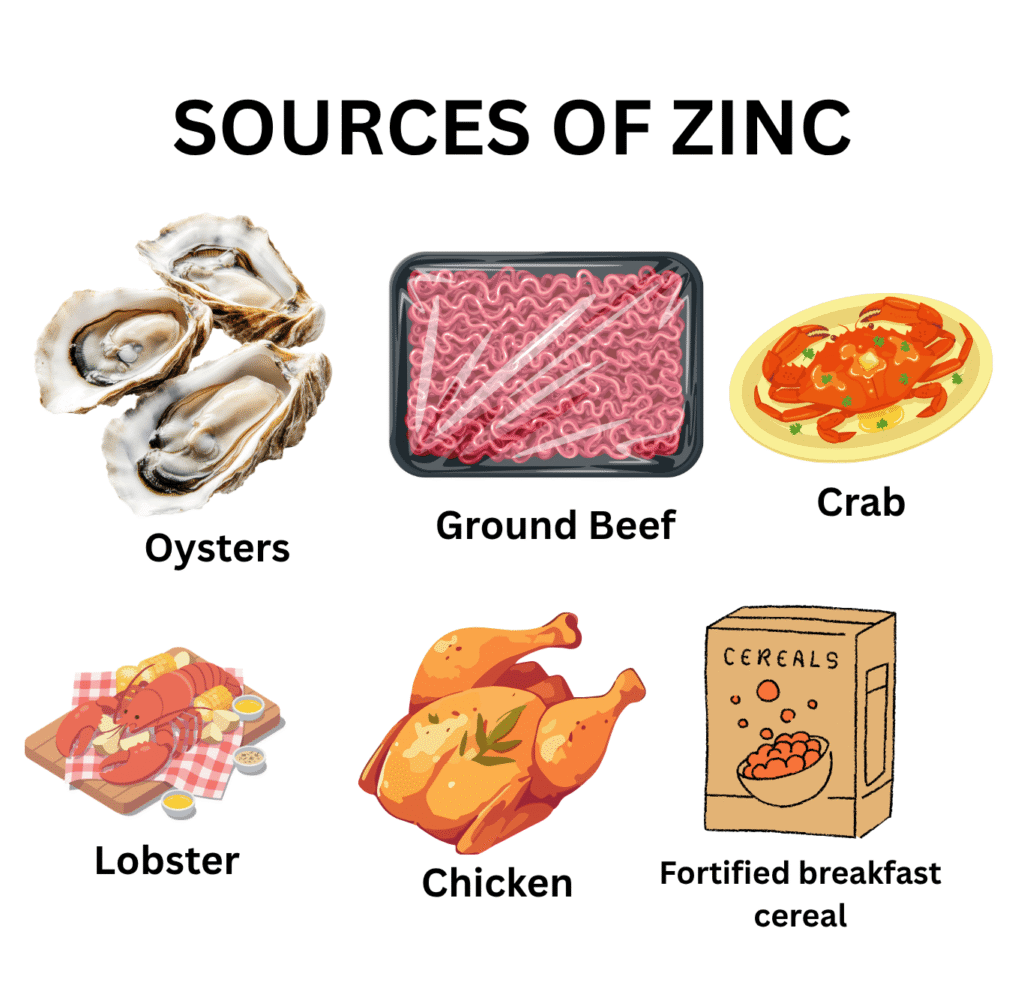
Best Food Sources of Zinc
Zinc bioavailability varies dramatically between food sources. How much you absorb depends as much on what else you eat with it as on how much is in the food itself.
|
Food Source |
Serving |
Zinc (mg) |
Bioavailability |
|
Oysters (cooked) |
85 g (3 oz) |
74 mg ✦ Highest |
Very high, haem matrix |
|
Beef (ground, cooked) |
85 g (3 oz) |
5.3 mg |
High,animal source |
|
Crab (cooked) |
85 g (3 oz) |
6.5 mg |
High |
|
Lobster (cooked) |
85 g (3 oz) |
3.4 mg |
High |
|
Pork chop (cooked) |
85 g (3 oz) |
2.9 mg |
High |
|
Chicken (dark meat, cooked) |
85 g (3 oz) |
2.4 mg |
Moderate |
|
Fortified breakfast cereal |
1 serving |
Up to 3.8 mg |
Moderate (check label) |
|
Pumpkin seeds |
28 g (1 oz) |
2.2 mg |
Lower, phytate inhibition |
|
Hemp seeds |
28 g (1 oz) |
3.0 mg |
Lower, phytate inhibition |
|
Chickpeas (cooked) |
½ cup (~82 g) |
1.3 mg |
Lowe, high phytate; soak and sprout to improve |
|
Cashews |
28 g (1 oz) |
1.6 mg |
Lower, phytate inhibition |
Table 6. Top dietary sources of zinc with bioavailability ratings. Source: NIH ODS / USDA FoodData Central. Adult men RDA = 11 mg/day; women = 8 mg/day.
🦪 Practical Note: One serving of oysters (85 g) provides approximately 74 mg of zinc, nearly 7× the adult male RDA. This is the single most zinc-dense food on the planet by far. For those who do not eat oysters, beef is the most practical everyday source of highly bioavailable zinc.
How to Prevent Zinc Deficiency: Strategies for Every Risk Group
For the General Population
- Include meat, shellfish, or poultry regularly. These provide the most bioavailable zinc.
- Eat a variety of zinc-containing plant foods alongside animal sources. The combination improves overall zinc status
- Soak, sprout, or ferment legumes and grains to reduce phytate inhibition
For Vegetarians and Vegans
- Deliberately plan zinc intake. Aim for 50% above the standard RDA to compensate for lower plant-food bioavailability
- Use phytate-reduction techniques consistently: soaking, sprouting, fermentation
- Consider a low-dose zinc supplement (15–25 mg elemental/day) – discuss with your doctor
- Annual serum zinc testing is reasonable
For Children in High-Risk Populations
- WHO recommendation: preventive zinc supplementation in children under 5 in populations with high zinc deficiency prevalence
- Dietary diversification from 6 months – introduction of zinc-rich complementary foods (meat, fish, eggs)
- Zinc supplementation as part of diarrhoea treatment, reduces duration and prevents recurrence.
For High-Risk Adults
- IBD patients: routine annual zinc testing; supplement if deficient; treat underlying IBD
- Post-bariatric surgery: lifelong zinc supplementation as part of micronutrient protocol; annual monitoring
- Heavy drinkers: zinc supplementation alongside other alcohol-related nutritional interventions
- Elderly (> 65 years): consider routine zinc supplementation: dietary intake typically inadequate, impaired absorption is common.
- Patients on loop diuretics: annual zinc monitoring alongside potassium and magnesium
Zinc Toxicity: The Copper Depletion Danger
Zinc toxicity from food is essentially impossible. Toxicity from supplements is real and clinically important. It is not because zinc itself is acutely dangerous at moderate doses, but because of what excess zinc does to another essential mineral, copper.
The Zinc-Copper Interaction
Zinc and copper compete for absorption via intestinal metallothionein. High zinc
- Induces metallothionein production in intestinal enterocytes
- Metallothionein preferentially binds copper
- Bound copper is trapped in the enterocyte and excreted when the cell dies
- Result: copper absorption is blocked even when dietary copper intake is adequate
Chronic copper depletion from excess zinc supplementation causes:
- Copper-deficiency anaemia: sideroblastic or normocytic, that does not respond to iron treatment
- Copper-deficiency myeloneuropathy: a subacute combined degeneration-like picture with gait ataxia and sensory loss
- Neutropenia: low white cell count
⚠️ Warning: Never supplement zinc above 40 mg elemental/day for more than a few weeks without monitoring serum copper and caeruloplasmin. The zinc-copper interaction is dose-dependent and cumulative. Copper-deficiency neuropathy is irreversible if treatment is delayed.
Acute Zinc Toxicity: GI Effects
- Nausea, vomiting, abdominal cramps: most common with doses > 50 mg elemental zinc at once
- Metallic taste in the mouth
- Diarrhoea
- These effects are dose-dependent and resolve when zinc is stopped or dose reduced
Zinc vs Iron vs Vitamin A Deficiency: How to Tell Them Apart
|
Feature |
Zinc Deficiency |
Iron Deficiency |
Vitamin A Deficiency |
|
Global prevalence |
17–31% of global population |
1.27 billion people |
190 million children under 5 |
|
Hallmark symptom |
Loss of taste and smell |
Fatigue, pallor, pica |
Night blindness, Bitot’s spots |
|
Anaemia? |
Normocytic (mild) in severe cases |
Microcytic, hypochromic |
No direct cause |
|
Key childhood impact |
Stunting, immune failure |
Cognitive impairment, fatigue |
Blindness, measles mortality |
|
Toxicity risk |
Yes, depletes copper at > 40 mg/day |
Iron overload possible (haemochromatosis) |
Yes. It is teratogenic in pregnancy |
|
Key diagnostic test |
Serum zinc (limited sensitivity) |
Serum ferritin |
Serum retinol |
Table 7. Comparative guide — Zinc vs Iron vs Vitamin A deficiency. Source: Clinical experience + NCBI StatPearls; NIH ODS.
Frequently Asked Questions About Zinc Deficiency
Related Articles on MedBeaconHub.com
- Nutritional Deficiency Diseases: A Doctor’s Complete Guide (Pillar Article)
- Iron Deficiency Anaemia: Why Iron and Zinc Often Fall Together
- Vitamin A Deficiency: Another Immune Mineral Partner
- Copper Deficiency: The Hidden Consequence of Excess Zinc
- Magnesium Deficiency: Another Trace Mineral Behind Immunity and Energy
- Folate Deficiency: Symptoms, Causes, Treatment and Prevention
References and Authoritative Sources
- NIH Office of Dietary Supplements — Zinc Fact Sheet for Health Professionals
- NCBI StatPearls — Zinc Deficiency (Updated August 2025)
- IFPRI — Addressing the Global, Life-Long Health Impacts of Zinc Deficiency: A Call to Action (2024)
- Nature Scientific Reports — Demographic and Clinical Characteristics of Zinc Deficiency: Nationwide Japanese Claims Database (2024)
- PMC — Zinc Deficiency as Possible Link Between Immunosenescence and Age-Related Diseases (May 2025)
- PMC Nutrients 2025 — Prevalence and Impact of Zinc Deficiency on Clinical Outcomes in Inflammatory Bowel Disease
- Cleveland Clinic — Zinc Deficiency: Symptoms, Causes and Treatment
- Merck Manual Professional Edition — Zinc Deficiency
- WHO — Zinc Supplementation in Management of Diarrhoea
- Advances in Nutrition 2024 — Preventing and Controlling Zinc Deficiency Across the Life Course: A Call to Action
