
Vitamin A Deficiency: Symptoms, Causes, Night Blindness, Treatment and Prevention: The Complete Doctor’s Guide
The leading cause of preventable childhood blindness in the world, and a deficiency that kills as surely as it blinds.
✍️ Written and reviewed by: Dr. Qazi Taqweemulhaq, FCPS Medicin. Professor of Medicine, Women Medical and Dental College, Abbottabad, Pakistan. Consultant Physician, 32 Years Clinical Experience
📅 Last Updated: May 2026 | References: WHO, UNICEF, NIH ODS, NCBI StatPearls, Merck Manual, The Lancet, Medscape, Cleveland Clinic
⚡ Quick Answer: Vitamin A deficiency (serum retinol < 0.70 µmol/L) is the world’s leading cause of preventable childhood blindness, affecting 190 million children under 5 globally. Night blindness is the earliest symptom. Bitot’s spots on the conjunctiva are pathognomonic. Severe deficiency causes keratomalacia, irreversible corneal destruction and blindness. Treatment uses the WHO massive-dose retinol protocol. CRITICAL: high-dose preformed Vitamin A is teratogenic: pregnant women must never exceed 3,000 mcg RAE/day.
|
✅ KEY TAKEAWAYS — Vitamin A Deficiency |
|
|
• Vitamin A deficiency is the world’s leading cause of preventable childhood blindness. 250,000–500,000 children go blind every year |
|
|
|
|
• Bitot’s spots on the conjunctiva are pathognomonic : white foamy triangular plaques that confirm Vitamin A deficiency on examination |
|
|
|
|
|
|
A Child Goes Blind Every Two Minutes. Almost Every Case Is Preventable.
I want to tell you about a five-year-old boy I will never forget. He came through a colleague’s referral, a child from a rural district. He had been brought to the city when his parents noticed something was wrong with his eyes.
They had noticed it gradually: at first, he seemed to stumble after sunset. He stopped playing outside in the evenings. When they described it, what they were describing was night blindness, the inability to see in dim light.
It is the earliest, most recognisable symptom of Vitamin A deficiency.
By the time he was examined, his condition had progressed. His corneas were hazy, ulcerated. He was at stage X3A of xerophthalmia, active corneal ulceration.
Aggressive treatment with high-dose Vitamin A was started immediately. One eye was saved. The other was permanently damaged.
That child had eaten rice and lentils almost exclusively for two years. No animal products, no orange or yellow vegetables, no fortified foods. His diet contained virtually no Vitamin A, and yet the deficiency was entirely preventable.
The WHO estimates that 250,000 to 500,000 children go blind from Vitamin A deficiency every year. Of those who go blind, approximately half die within 12 months. This is because the immune failure that comes with severe Vitamin A deficiency makes them unable to survive common childhood infections. Vitamin A deficiency is not simply a disease of the eyes. It is a disease of survival.
Deficiencies in iron, Vitamin A, and iodine are the most common around the world, particularly in children and pregnant women. Yet Vitamin A deficiency receives far less attention than its burden justifies.
It disproportionately affects children in low-income settings, and because the solution.
This article is the complete clinical guide: what Vitamin A does, how to recognise deficiency at every stage before it becomes irreversible, how to treat it correctly, and how to prevent it. It is written for parents, for physicians, for anyone who wants to understand one of the world’s great preventable tragedies.
🏥 From My Clinic: I see subclinical Vitamin A deficiency in my practice, not the blinding form, but the immune form. Children with recurrent chest infections and persistent diarrhoea who are not thriving. Adults with persistent dry skin and night driving difficulty they attribute to ‘weak eyes.’
Once Vitamin A status is assessed and corrected, the improvement in infection frequency is often dramatic. Vitamin A is not only about eyes. It is also about immunity.
Once Vitamin A status is assessed and corrected, the improvement in infection frequency is often dramatic. Vitamin A is not only about eyes. It is also about immunity.
What Is Vitamin A and What Does It Do?
Vitamin A is a fat-soluble vitamin that exists in two main dietary forms:
- Preformed Vitamin A (retinol): found in animal products: liver, eggs, dairy, oily fish. This form is biologically active immediately. Stored in the liver. Can cause toxicity if in excess. It is especially dangerous in pregnancy.
- Provitamin A carotenoids (especially beta-carotene): found in orange, yellow, and dark green plant foods. Converted to retinol in the body as needed. Cannot cause Vitamin A toxicity regardless of intake, the conversion is self-limiting.
Both forms are measured in Retinol Activity Equivalents (RAE): a unit that accounts for the different bioactivity of preformed versus plant-derived Vitamin A.
1 mcg RAE = 1 mcg retinol = 12 mcg beta-carotene from food.
The Six Critical Functions of Vitamin A
- Vision, the most well-known role: Retinol is converted to retinal, which combines with opsin protein to form rhodopsin. This photosensitive pigment in the rod cells of the retina enables vision in low-light conditions. Deficiency depletes rhodopsin → night blindness.
- Epithelial integrity: Retinoic acid (the active hormonal form) regulates the differentiation of epithelial cells throughout the body: skin, cornea, conjunctiva, respiratory mucosa, GI lining, urinary tract. Deficiency causes squamous metaplasia, normal moist, functional epithelium is replaced by dry, keratinised cells that cannot perform their barrier function.
- Immune function: Vitamin A is essential for the proliferation and differentiation of all immune cells: T and B lymphocytes, natural killer cells, macrophages, and neutrophils. It also maintains mucosal barrier integrity, the first line of defence against pathogens.
Deficiency dramatically increases susceptibility to measles, diarrhoeal disease, and respiratory infection. - Gene regulation: Retinoic acid binds to nuclear receptors (RAR and RXR) and regulates the expression of hundreds of genes controlling cell growth, differentiation, and programmed cell death (apoptosis). This explains Vitamin A’s role in cancer prevention.
- Embryonic development and reproduction: Retinoic acid is essential for the development of the heart, lungs, kidneys, eyes, and limbs in the foetus. Both deficiency AND excess cause severe developmental abnormalities making the dosing range in pregnancy critically important.
- Bone health: Vitamin A is required for normal osteoblast and osteoclast activity, the cells that build and remodel bone. Paradoxically, both deficiency and excess impair bone health.
How Much Vitamin A Do You Need Per Day?
Requirements are expressed in mcg RAE (Retinol Activity Equivalents). The Upper Tolerable Intake Limit applies to preformed Vitamin A only, retinol from supplements and animal foods. Beta-carotene from plant foods has no upper limit.
|
Life Stage / Group |
RDA (mcg RAE/day) |
Upper Limit – Preformed Vit A Only (mcg/day) |
|
Infants 0–6 months |
400 mcg (AI) |
600 mcg |
|
Infants 7–12 months |
500 mcg (AI) |
600 mcg |
|
Children 1–3 years |
300 mcg |
600 mcg |
|
Children 4–8 years |
400 mcg |
900 mcg |
|
Children 9–13 years |
600 mcg |
1,700 mcg |
|
Men ≥19 years |
900 mcg RAE |
3,000 mcg |
|
Women ≥19 years |
700 mcg RAE |
3,000 mcg |
|
Pregnant women 19+ years |
770 mcg RAE |
3,000 mcg CRITICAL: exceeding this is teratogenic |
|
Lactating women 19+ years |
1,300 mcg RAE |
3,000 mcg |
Table 1. Vitamin A RDA and Upper Intake Levels. Source: NIH ODS; NCBI StatPearls (Updated February 2025). 1 mcg RAE = 3.33 IU of preformed Vitamin A.
⚠️ Warning: In pregnancy, the upper limit is critically important, 3,000 mcg RAE/day (10,000 IU/day). Exceeding this causes severe foetal malformations. Pregnant women should not take high-dose retinol supplements. Beta-carotene supplements are safe alternatives if dietary Vitamin A is inadequate.
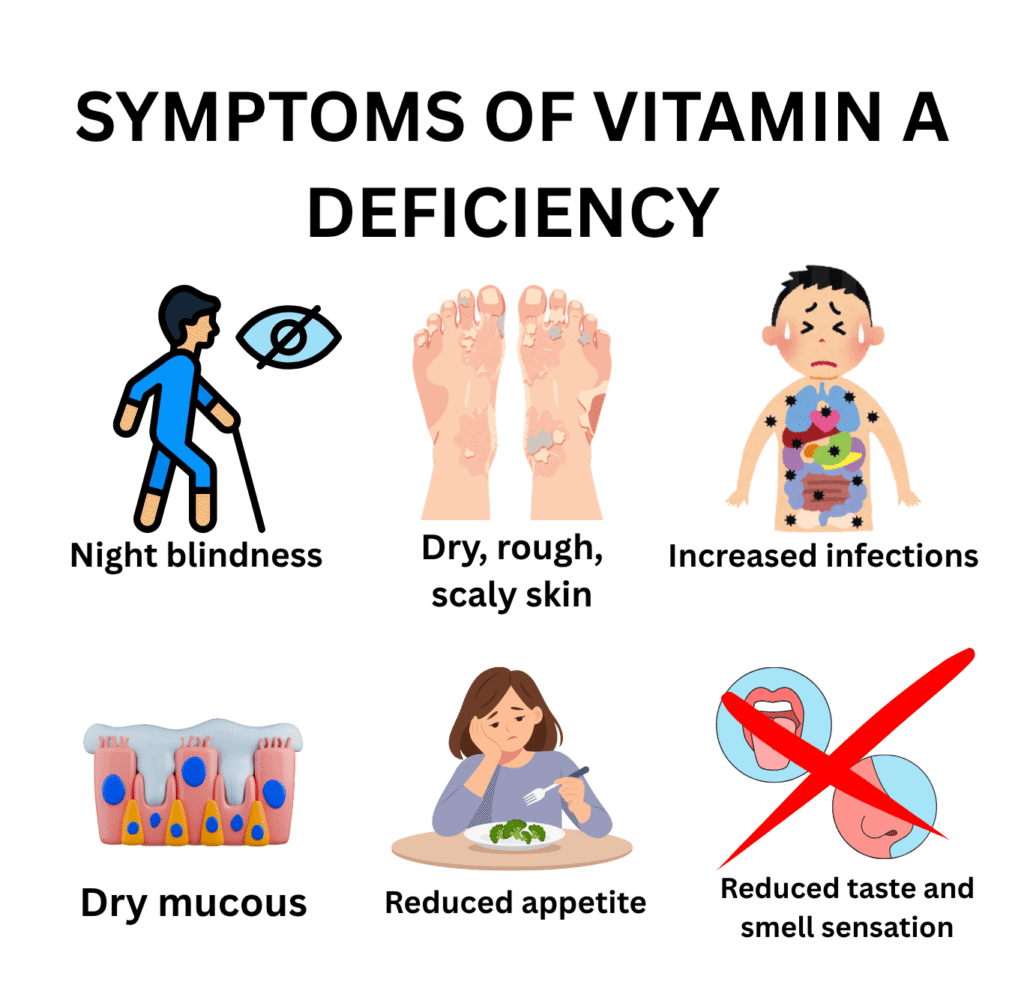
Vitamin A Deficiency Symptoms: From Night Blindness to Irreversible Blindness
The clinical spectrum of Vitamin A deficiency spans from subtle visual impairment to irreversible corneal destruction and death.
Early stages are completely reversible; late stages are not. Recognising deficiency before it reaches corneal involvement is the defining clinical challenge.
|
System |
Mild–Moderate Deficiency |
Severe / Prolonged Deficiency |
|
Eyes / Vision |
Night blindness, difficulty seeing in dim light or at dusk |
Conjunctival xerosis, Bitot’s spots, corneal xerosis, corneal ulceration, keratomalacia: irreversible blindness |
|
Skin |
Dry, rough, scaly skin (phrynoderma ‘toad skin’) |
Follicular hyperkeratosis: keratotic papules around hair follicles; extreme skin dryness |
|
Immunity |
Increased susceptibility to infections, especially respiratory and diarrhoeal |
Dramatically increased severity of measles, pneumonia, and diarrhoea: major cause of child mortality |
|
Mucous membranes |
Dry mucous membranes: mouth, nose, throat, airways |
Squamous metaplasia of respiratory and GI epithelium – increased infection risk |
|
Growth |
Slow growth, reduced appetite |
Stunting, wasting, failure to thrive in children |
|
Reproductive |
Night blindness in pregnancy (early sign of deficiency in pregnant women) |
Increased maternal mortality, preterm birth, low birth weight, foetal malformation risk |
|
Taste and smell |
Reduced taste and smell sensation |
Further reduces appetite and dietary intake perpetuating the deficiency |
Table 2. Vitamin A deficiency symptoms by severity and organ system. Sources: WHO; NCBI StatPearls; Merck Manual; Cleveland Clinic.
Night Blindness, The First Warning Sign
Night blindness, the inability to see in dim light or adapt to darkness after coming from a bright environment is the earliest and most reversible clinical sign of Vitamin A deficiency. In children:
- Stumbling or falling after dark
- Refusing to go outdoors in the evening
- Not recognising familiar faces or objects in low light
In pregnant women, night blindness is a recognised clinical indicator of Vitamin A deficiency and is associated with significantly increased maternal mortality risk.
💡 Clinical Insight: Night blindness (nyctalopia) in a child from a low-income background with a diet lacking animal products and coloured vegetables is Vitamin A deficiency until proven otherwise. Treat the same day. Do not wait for a blood result.
Skin Changes: Phrynoderma (‘Toad Skin’)
Vitamin A deficiency causes characteristic skin changes:
- Phrynoderma: dry, rough, scaly skin with follicular hyperkeratosis, keratotic papules around hair follicles that give the skin a ‘toad-like’ texture
- Most prominent on the extensor surfaces of the thighs, upper arms, and buttocks
- Occurs because retinoic acid is required for normal keratinocyte differentiation. Without it, skin cells fail to mature correctly.
Immune Failure, The Hidden Killer
Vitamin A is sometimes called the ‘anti-infection vitamin’ and for good reason. Deficiency impairs immunity through multiple mechanisms:
- Loss of mucosal barrier integrity → pathogens penetrate respiratory and GI epithelium more easily
- Reduced lymphocyte proliferation → weakened adaptive immune response
- Impaired neutrophil function → reduced bacterial killing capacity
The result: Vitamin A-deficient children are dramatically more likely to die from measles, pneumonia, and diarrhoea, the three leading infectious causes of childhood death in low-income countries. Vitamin A supplementation reduces all-cause child mortality by 12–24% (UNICEF 2023 data).
The Xerophthalmia Staging System: From Reversible to Irreversible
Xerophthalmia is the clinical spectrum of ocular manifestations of Vitamin A deficiency, from the earliest reversible stage to irreversible blindness. The WHO classification system is the gold standard for grading severity and guiding treatment urgency.
|
WHO Stage |
Clinical Finding |
Description and Significance |
|
XN |
Night blindness |
Earliest reversible sign. Child cannot see in dim light or at dusk. Reversible with treatment |
|
X1A |
Conjunctival xerosis |
Conjunctiva loses its normally moist, glistening appearance. Becomes dry and dull |
|
X1B |
Bitot’s spots |
Pathognomonic white, foamy, triangular plaques on the temporal conjunctiva. Caused by keratin accumulation. Confirm Vitamin A deficiency |
|
X2 |
Corneal xerosis |
Cornea becomes dry, hazy, and loses lustre. Urgent treatment required. Progression to blindness is rapid |
|
X3A |
Corneal ulceration (< ½ surface) |
Corneal ulcers develop. Medical emergency. Immediate high-dose Vitamin A treatment required. Risk of irreversible blindness |
|
X3B |
Keratomalacia (> ½ surface) |
Corneal necrosis and liquefaction. IRREVERSIBLE blindness results. Even with treatment, vision cannot be restored. Prevention is the only answer |
|
XS |
Corneal scar |
Healed stage. Permanent corneal opacity causing varying degrees of visual impairment |
|
XF |
Xerophthalmic fundus |
Retinal changes visible on fundoscopy, associated with severe or prolonged deficiency |
Table 3. WHO Xerophthalmia Classification System. Sources: WHO; Merck Manual; NCBI StatPearls. Note: stages X2 and above are medical emergencies requiring same-day high-dose Vitamin A treatment.
Bitot’s Spots: The Pathognomonic Sign
Bitot’s spots are white, foamy, triangular plaques on the temporal (outer) conjunctiva: one of the most distinctive signs in all of nutritional medicine. They are:
- Caused by accumulation of keratin debris from squamous metaplasia of the conjunctival epithelium
- Foamy appearance from gas-producing bacteria colonising the keratinised surface
- Triangular in shape, with the base at the limbus
- Pathognomonic for Vitamin A deficiency – no other condition produces this sign
In a child from a high-risk population, Bitot’s spots confirm the diagnosis clinically. Treatment should begin the same day.
Keratomalacia: When Blindness Becomes Inevitable
Keratomalacia is the most feared complication of Vitamin A deficiency: corneal necrosis and liquefaction that destroys the eye’s optical surface. At this stage:
- The cornea becomes soft, necrotic, and may perforate
- Even with immediate high-dose Vitamin A treatment, the visual loss is permanent
- The eye may be lost entirely if infection supervenes
Keratomalacia does not sneak up unannounced. It is always preceded by earlier, recognisable, reversible stages. This is why early detection and treatment of night blindness and Bitot’s spots is so clinically important.
⚠️ Warning: Corneal involvement (X2 and above) is a medical emergency.
High-dose Vitamin A treatment must be started the same day.
Do not wait for laboratory confirmation.
The window for preventing irreversible blindness is narrow.
What Causes Vitamin A Deficiency? Every Cause Explained
|
Cause |
Specific Cause |
Key Mechanism |
|
Dietary |
Low intake of animal products and orange/yellow vegetables |
Most common cause. Diets relying primarily on rice, cassava, or maize with minimal fat contain negligible Vitamin A. |
|
Malabsorption |
Fat malabsorption: coeliac, IBD, cystic fibrosis, chronic pancreatitis, cholestatic liver disease |
Vitamin A is fat-soluble. It requires dietary fat and bile for absorption. Any condition causing fat malabsorption causes Vitamin A malabsorption |
|
Liver disease |
Cirrhosis, alcoholic liver disease, hepatitis |
Liver stores 90% of total body Vitamin A. Liver disease impairs storage, conversion of carotenoids to retinol, and production of retinol-binding protein (RBP). |
|
Protein deficiency |
Kwashiorkor, severe protein-energy malnutrition |
Retinol-binding protein (RBP) is a protein required to transport Vitamin A in the blood. Protein deficiency impairs RBP production even if Vitamin A stores are present, it cannot be delivered to tissues |
|
Increased demand |
Pregnancy and lactation |
Vitamin A transfer to foetus and in breast milk dramatically increases maternal demand. Night blindness in pregnancy is a recognised clinical indicator of deficiency. |
|
Infection |
Measles, diarrhoeal disease, respiratory infections |
Infections dramatically increase Vitamin A utilisation and urinary losses. Measles is both caused and worsened by Vitamin A deficiency, a vicious cycle. |
|
Bariatric surgery |
Gastric bypass, sleeve gastrectomy |
Bypasses proximal small intestine where fat-soluble vitamin absorption occurs. Vitamin A deficiency is common post-bariatric surgery if not supplemented |
Table 4. Complete causes of Vitamin A deficiency. Sources: WHO; NIH ODS; NCBI StatPearls; Merck Manual.
The Measles-Vitamin A Vicious Cycle
The relationship between measles and Vitamin A deficiency is one of the most clinically important interactions in infectious disease medicine:
- Vitamin A deficiency dramatically increases susceptibility to measles and its severity
- Measles infection dramatically depletes Vitamin A stores through fever-induced catabolism and reduced dietary intake
- Post-measles Vitamin A deficiency can rapidly progress to corneal ulceration and blindness
- High-dose Vitamin A given during measles reduces measles mortality by 50–80% in deficient populations
💡 Clinical Insight: The WHO recommends high-dose Vitamin A supplementation for all children with measles in countries where Vitamin A deficiency is a public health problem including Pakistan. If you are treating a child with measles in a high-risk area, give Vitamin A on the first two days of treatment. This is potentially life-saving.
How Is Vitamin A Deficiency Diagnosed?
Diagnosis is primarily clinical in resource-limited settings, based on dietary history, physical examination, and ocular findings. Blood tests confirm the diagnosis but should not delay treatment when clinical signs are present.
Clinical Assessment
- Dietary history: animal product intake, orange/yellow vegetable intake, fortified food consumption, breastfeeding status
- Ocular examination: night blindness history; slit-lamp examination for conjunctival xerosis, Bitot’s spots, corneal changes
- Skin examination: phrynoderma, follicular hyperkeratosis on extensor surfaces
- General nutritional assessment: weight-for-height, mid-upper arm circumference, co-existing protein-energy malnutrition
Laboratory Tests
- Serum retinol (gold standard): Deficiency: < 0.70 µmol/L (< 20 µg/dL). Marginal deficiency: 0.70–1.05 µmol/L. Note: serum retinol is homeostatically regulated and may not reflect liver stores accurately until severely depleted.
- Modified relative dose response (MRDR): measures liver Vitamin A reserves more accurately, mainly for research purpose.
- Retinol-binding protein (RBP): reflects Vitamin A transport status; falls in deficiency but also falls in infection and protein malnutrition
- Conjunctival impression cytology: goblet cell density reflects Vitamin A status at the conjunctival level, used in population surveys
💡 Clinical Insight: In clinical practice, a child with night blindness, Bitot’s spots, or phrynoderma in a high-risk nutritional environment should receive Vitamin A treatment immediately, without waiting for laboratory confirmation. The test is valuable for population surveys and monitoring; the treatment decision in an individual child should be based on the clinical picture.
Vitamin A Deficiency Treatment: The WHO Supplementation Protocol
Treatment follows the WHO Massive Dose Vitamin A Protocol, a three-dose schedule that rapidly replenishes depleted liver stores. The protocol uses oral retinyl palmitate or retinyl acetate, oil-based formulations with the best bioavailability.
|
Clinical Scenario |
WHO Treatment Protocol |
Notes |
|
Deficiency with xerophthalmia (children > 1 year and adults) |
200,000 IU oral retinol on Day 1, Day 2, and Day 8–14 |
The WHO Massive Dose protocol. Three doses over two weeks to rapidly replenish liver stores |
|
Infants 6 -12 months with xerophthalmia |
100,000 IU oral retinol on Day 1, Day 2, and Day 8–14 |
Half the adult dose. Immediate treatment is essential to prevent irreversible blindness |
|
Infants < 6 months with xerophthalmia |
50,000 IU oral retinol on Day 1, Day 2, and Day 8–14 |
Quarter dose for neonates and young infants |
|
Measles in areas of high VAD prevalence |
200,000 IU on 2 consecutive days |
WHO recommends Vitamin A for all children with measles in at-risk populations. Reduces measles mortality by 50–80%. |
|
Pregnant women with night blindness |
Weekly low-dose Vitamin A (up to 10,000 IU/week) OR beta-carotene equivalent |
NEVER give high-dose retinol in pregnancy: teratogenic risk. Low-dose weekly or beta-carotene are safe alternatives |
|
Post-bariatric surgery (prevention) |
Retinol supplement 5,000–10,000 IU/day with fat-containing meal |
Lifelong supplementation required. Annual serum retinol monitoring |
|
Subclinical deficiency (dietary cause) |
Dietary optimisation, increase orange/yellow vegetables, animal products, fortified foods |
Supplements needed only if dietary improvement is insufficient or malabsorption is present |
Table 5. WHO Vitamin A treatment protocol. Sources: WHO Guidelines; NCBI StatPearls (February 2025); Merck Manual (June 2025).
Response to Treatment, What to Expect
- Night blindness: improves within 24–48 hours of the first dose, the fastest response in nutritional medicine
- Conjunctival xerosis and Bitot’s spots: begin resolving within 1–2 weeks
- Corneal xerosis (X2): may partially reverse with aggressive treatment, outcome variable
- Corneal ulceration (X3A/X3B): visual loss is permanent even with treatment. Topical antibiotics and lubricants used to prevent secondary infection.
- Immunity and infection frequency: improves over 4–8 weeks of restored Vitamin A status
- Skin changes (phrynoderma): resolves gradually over months
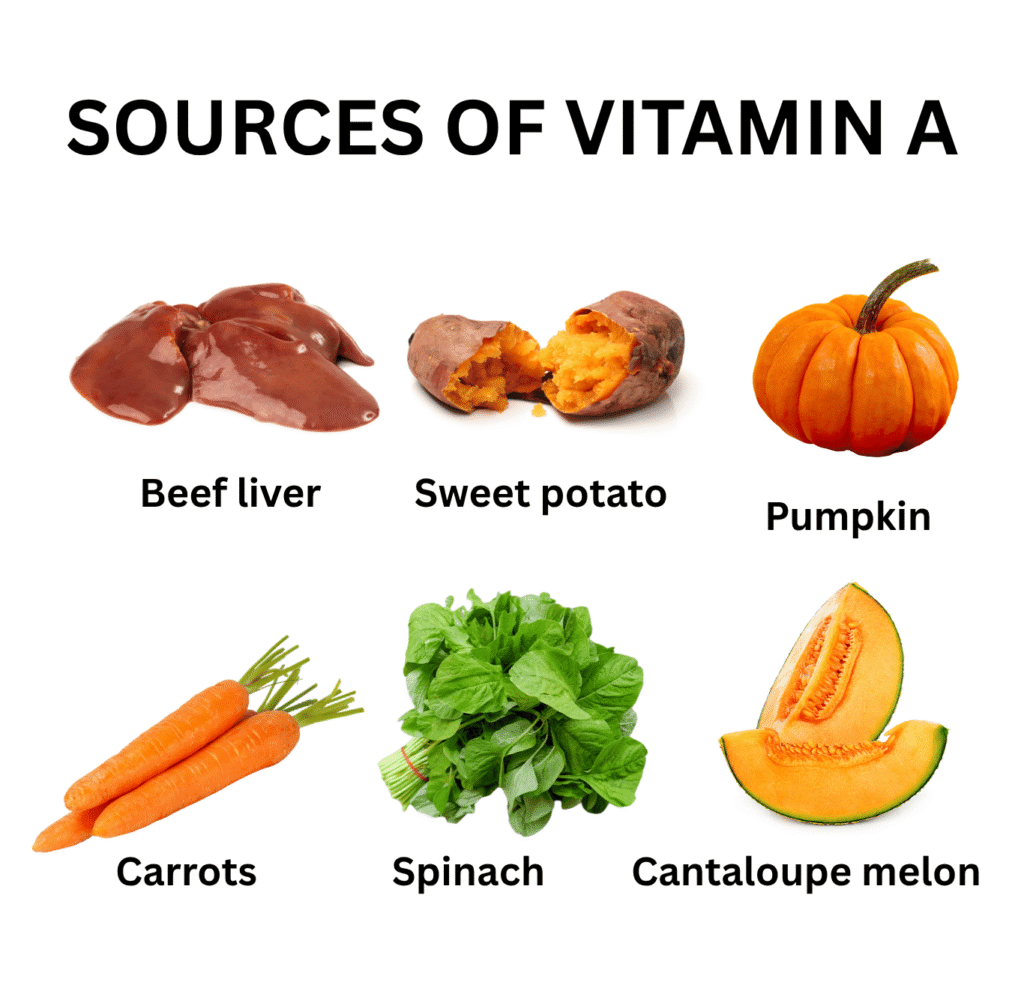
Best Food Sources of Vitamin A: Preformed and Provitamin A
Vitamin A is obtained from two dietary categories, preformed retinol from animal products, and provitamin A carotenoids from plant foods. Both contribute to Vitamin A status, but with important differences in bioavailability and safety.
|
Food Source |
Serving |
Vitamin A (mcg RAE) |
Type |
|
Beef liver (cooked) |
85 g (3 oz) |
6,582 mcg ✦ Highest |
Preformed retinol, exceeds UL. Eat weekly, not daily |
|
Sweet potato (baked) |
1 medium (~130 g) |
961 mcg RAE |
Provitamin A (beta-carotene) |
|
Pumpkin (cooked) |
½ cup (~123 g) |
953 mcg RAE |
Provitamin A (beta-carotene) |
|
Carrots (raw) |
½ cup (~61 g) |
459 mcg RAE |
Provitamin A (beta-carotene) |
|
Spinach (cooked) |
½ cup (~90 g) |
472 mcg RAE |
Provitamin A |
|
Cantaloupe melon |
½ cup cubed (~80 g) |
135 mcg RAE |
Provitamin A |
|
Egg (hard-boiled) |
1 large |
75 mcg RAE |
Preformed retinol |
|
Salmon (cooked) |
85 g (3 oz) |
59 mcg RAE |
Preformed retinol |
|
Whole milk |
1 cup (240 ml) |
112 mcg RAE |
Preformed retinol |
|
Mango (raw) |
½ cup (~83 g) |
45 mcg RAE |
Provitamin A |
Table 6. Top dietary sources of Vitamin A. Source: NIH ODS / USDA FoodData Central. Adult men RDA = 900 mcg RAE/day; women = 700 mcg RAE/day.
Key Dietary Principles
- Eat fat with provitamin A foods: beta-carotene from vegetables requires dietary fat for absorption. A carrot salad with olive oil absorbs significantly more beta-carotene than a fat-free salad.
- Cook orange and yellow vegetables: cooking breaks down cell walls and increases beta-carotene bioavailability from most vegetables
- Limit liver to weekly: beef liver is extraordinarily rich in preformed Vitamin A. One serving provides 7× the daily RDA. Eating it more than once a week chronically risks toxicity, especially in women who may become pregnant.
- Breast milk is protective: breast milk contains Vitamin A. Exclusively breastfed infants of well-nourished mothers are protected. Maternal Vitamin A deficiency directly impairs breast milk Vitamin A content.
How to Prevent Vitamin A Deficiency
For Children (High-Risk Populations)
- WHO Vitamin A Supplementation Programme: high-dose supplements every 6 months for all children aged 6–59 months in at-risk countries. UNICEF reports 75% coverage of targeted children in 2023.
- Exclusive breastfeeding for 6 months: breast milk provides adequate Vitamin A for well-nourished mothers’ infants
- Dietary diversification: introduction of orange and yellow vegetables, eggs, and dairy from 6 months of age
- Food fortification: sugar, cooking oil, and flour fortified with Vitamin A in many countries
- Measles vaccination: prevents measles-associated Vitamin A depletion, one of the most cost-effective child health interventions
For Pregnant Women
- Increase dietary Vitamin A through beta-carotene-rich foods: sweet potato, pumpkin, carrots, dark leafy greens, mango
- Prenatal supplements with Vitamin A: standard prenatal vitamins contain safe levels (770 mcg RAE). Do not exceed 3,000 mcg RAE/day total
- In areas of endemic Vitamin A deficiency: WHO recommends weekly low-dose supplementation (up to 10,000 IU/week) NOT high-dose single doses
- Monitor for night blindness: night blindness in pregnancy is a clinical indicator of deficiency. Report it to your physician immediately
For the General Population in High-Income Countries
- A varied diet including dairy, eggs, oily fish, and orange/yellow vegetables provides adequate Vitamin A for most people
- Avoid high-dose retinol supplements unless prescribed. The UL of 3,000 mcg RAE/day is easily exceeded by combined food and supplement intake
- Post-bariatric surgery patients: lifelong Vitamin A supplementation under medical supervision
Vitamin A Toxicity: A Real and Serious Risk
Unlike most other vitamins, Vitamin A specifically preformed retinol has a narrow therapeutic window. It is stored in the liver and accumulates. Toxicity is real and documented.
|
Type |
When It Occurs |
Symptoms |
|
Acute toxicity |
Single very high dose > 150 mg (500,000 IU) in adults |
Nausea, vomiting, headache, dizziness, blurred vision, skin peeling: resolves within days of stopping |
|
Chronic toxicity (Hypervitaminosis A) |
Prolonged daily intake > 3,000 mcg RAE (10,000 IU) for months |
Liver damage, alopecia, bone and joint pain, skin changes (dry, peeling), headache, raised intracranial pressure, hypercalcaemia |
|
Teratogenicity |
Any dose > 3,000 mcg RAE/day during pregnancy |
Severe birth defects: craniofacial, cardiac, and CNS malformations. Even at 7,500–10,000 IU/day, foetal risk is documented |
|
Beta-carotene — NO TOXICITY |
Beta-carotene from food or supplements cannot cause Vitamin A toxicity |
Excess beta-carotene causes carotenodermia (orange skin discolouration) – harmless and reversible. Safe in pregnancy |
Table 7. Vitamin A toxicity types and thresholds. Sources: NCBI StatPearls Vitamin A Toxicity (September 2023); NIH ODS; Merck Manual.
The Isotretinoin Warning
Isotretinoin, a synthetic retinoid used for severe acne is one of the most potent human teratogens known. Even a single course taken during pregnancy causes severe foetal malformation. Every prescriber of isotretinoin must ensure pregnancy prevention protocols (iPLEDGE in the USA) are strictly followed. This is not a theoretical risk, it is documented in thousands of cases.
💡 Clinical Insight: Beta-carotene from food carries no toxicity risk regardless of quantity. Carotenodermia (orange skin) from very high carrot or sweet potato intake is harmless and fully reversible. Never restrict plant-based Vitamin A sources for fear of toxicity – only preformed retinol supplements carry this risk.
Vitamin A vs Vitamin D vs Vitamin C Deficiency – How to Tell Them Apart
|
Feature |
Vitamin A Deficiency |
Vitamin D Deficiency |
Vitamin C Deficiency |
|
Primary deficiency population |
Children in low-income countries |
Global, all ages |
Elderly, smokers, restricted diets |
|
Hallmark symptom |
Night blindness; Bitot’s spots |
Bone pain; muscle weakness |
Bleeding gums; corkscrew hairs |
|
Blindness risk? |
Yes, leading preventable cause |
No |
No |
|
Child mortality link? |
Yes, measles, diarrhoea deaths |
Indirect |
If severe (scurvy) |
|
Toxicity risk in pregnancy? |
High, teratogenic above 3,000 mcg/day |
Low at normal supplemental doses |
Very low |
|
Key diagnostic test |
Serum retinol (< 0.70 µmol/L = deficient) |
Serum 25(OH)D |
Serum ascorbic acid |
Table 8. Comparative guide — Vitamin A vs D vs C deficiency. Source: Clinical experience + WHO; NCBI StatPearls; NIH ODS.
Frequently Asked Questions About Vitamin A Deficiency
Related Articles on MedBeaconHub.com
- Nutritional Deficiency Diseases: A Doctor’s Complete Guide (Pillar Article)
- Vitamin D Deficiency: Another Fat-Soluble Vitamin With Major Consequences
- Zinc Deficiency: The Immune Mineral That Works Alongside Vitamin A
- Iron Deficiency Anaemia: Why Iron and Vitamin A Often Fall Together
- Vitamin C Deficiency (Scurvy): Symptoms, Causes and Treatment
References and Authoritative Sources
- WHO — Vitamin A Deficiency
- UNICEF — Vitamin A Deficiency in Children (Updated September 2025)
- NIH Office of Dietary Supplements — Vitamin A and Carotenoids: Fact Sheet for Health Professionals (Updated December 2023)
- NCBI StatPearls — Vitamin A (Updated February 2025)
- NCBI StatPearls — Vitamin A Toxicity (Updated September 2023)
- Merck Manual Professional Edition — Vitamin A Deficiency (Updated June 2025)
- Medscape — Vitamin A Deficiency Treatment and Management (Updated February 2025)
- The Lancet Global Health — Trends and Mortality Effects of Vitamin A Deficiency in 138 Countries 1991–2013
- PMC — Comprehensive Analysis of Vitamin A Deficiency Burden: GBD 2021 and Predictions to 2050
- Frontiers in Nutrition 2024 — Clinical Vitamin A Deficiency Among Preschool Children in Southwest Ethiopia