
Magnesium Deficiency: Symptoms, Causes, Best Supplement Forms, Treatment and Prevention – The Complete Doctor’s Guide
The mineral that controls over 300 body processes — and that almost half of us are not getting enough of
✍️ Written and reviewed by: Dr. Qazi Taqweemulhaq, FCPS Medicine — Professor of Medicine, Women Medical and Dental College, Abbottabad, Pakistan. Consultant Physician, 32 Years Clinical Experience
📅 Last Updated: May 2026 | References: NIH ODS, NCBI StatPearls, Open Heart PMC, Frontiers in Nutrition, IJVNR 2025, Cleveland Clinic, Merck Manual
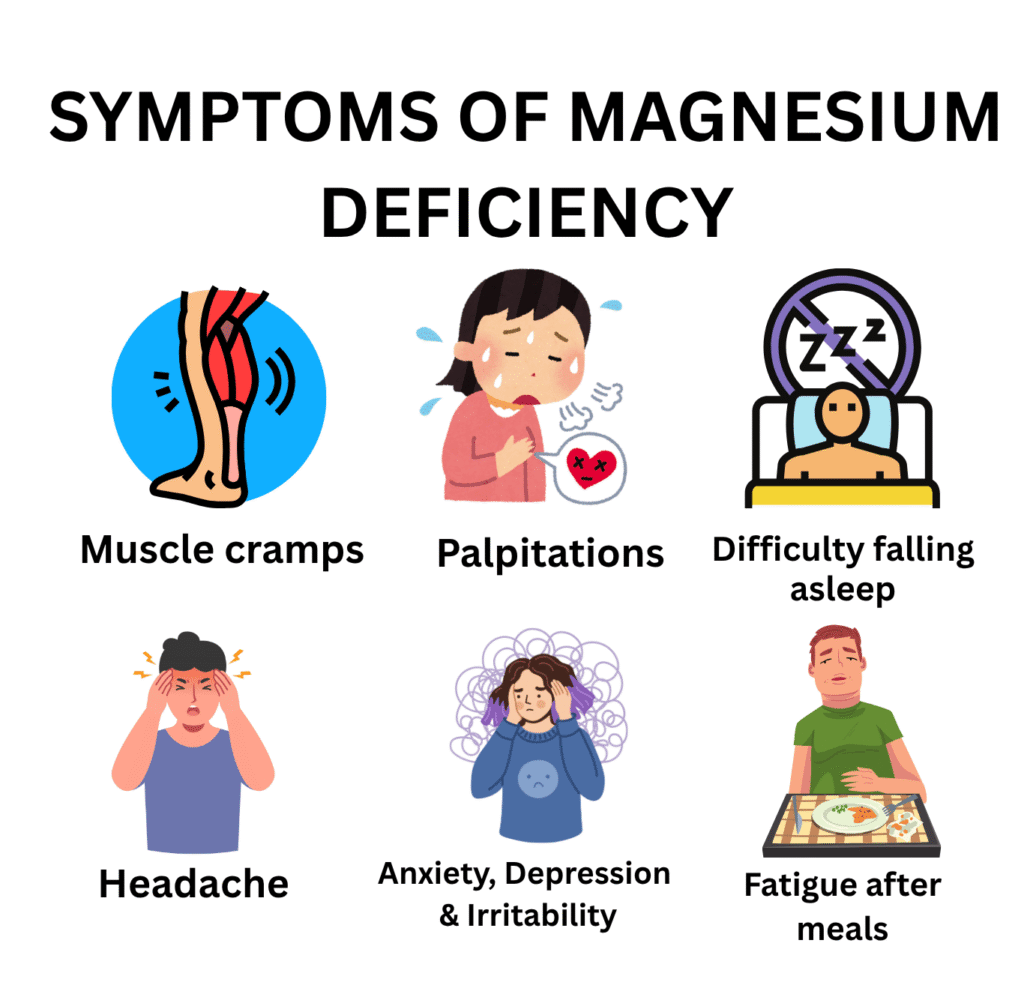
⚡ Quick Answer: Magnesium deficiency (hypomagnesaemia) affects 2.4 billion people, 31% of the global population. It causes muscle cramps, insomnia, anxiety, palpitations, headaches, and in severe cases life-threatening cardiac arrhythmias and seizures. The most common causes are poor diet, type 2 diabetes, loop diuretics, proton pump inhibitors, and alcohol use. Serum magnesium is an unreliable marker, intracellular stores can be depleted while serum appears normal. Best treatment: magnesium glycinate or citrate for most patients; IV magnesium sulphate for emergencies.
|
✅ KEY TAKEAWAYS — Magnesium Deficiency |
|
• Magnesium deficiency affects 2.4 billion people, 31% of the global population. Up to 50% of Americans fall short of the daily requirement. |
|
• Serum magnesium is a poor marker of true body stores, levels can appear ‘normal’ while intracellular stores are significantly depleted. |
|
• Magnesium is required to ACTIVATE Vitamin D. Deficiency of magnesium can prevent your Vitamin D supplement from working. |
|
• Refractory hypokalaemia and hypocalcaemia (potassium/calcium that will not correct) are almost always caused by undetected magnesium deficiency. |
|
• PPIs (omeprazole, lansoprazole) carry an FDA warning for hypomagnesaemia. Every patient on long-term PPIs needs annual magnesium monitoring. |
|
• Magnesium oxide (the most commonly sold form) has only 4% absorption, buy magnesium glycinate or citrate instead |
You Are Probably Low in Magnesium Right Now – And You Almost Certainly Do Not Know It.
I want to start with a number that stopped me in my tracks when I first saw the research: 2.4 billion people, approximately 31% of the entire global population consume inadequate magnesium every single day. In the United States alone, 45 to 50% of Americans fall below the recommended daily intake.
Magnesium is not a rare, exotic mineral. It is the fourth most abundant cation in the human body. It is a cofactor in over 300 enzymatic reactions. It is required for ATP production which means every cell in your body needs it to generate energy. It also activates Vitamin D, a patient can take Vitamin D supplements faithfully every day and still not benefit from them if their magnesium is insufficient.
Despite all of this, magnesium deficiency is chronically underdiagnosed for two reasons:
- Symptoms are non-specific: fatigue, muscle cramps, poor sleep, anxiety, easy to attribute to stress or ageing
- Serum magnesium is a poor marker of true body stores, less than 1% of the body’s magnesium is in the blood. Serum levels can appear normal while intracellular and bone magnesium are significantly depleted
I want to ask you some questions:
- Do you wake at night with cramps in your legs?
- Do you feel anxious for no clear reason?
- Is your sleep light, broken, or unrefreshing?
- Do you get frequent headaches or migraines?
- Are you on a loop diuretic, a PPI, or do you have type 2 diabetes?
If you answered yes to any of those, magnesium deficiency belongs in your differential diagnosis.
🏥 From My Clinic: A 48-year-old woman came to me ‘falling apart.’ Leg cramps every night. Palpitations labelled ‘benign ectopics.’ Anxiety not responding to SSRIs (the medicines for anxiety). Poor sleep for years. Her serum magnesium was 0.62 mmol/L, mildly deficient. But she was on omeprazole for reflux and furosemide for mild leg oedema. Two drugs silently draining her magnesium every day. We stopped the furosemide, switched to an H2 blocker (stomach acid reducing medicine but not PPI), and started magnesium glycinate 400 mg daily. Within six weeks, the cramps had stopped, the palpitations had disappeared, her sleep had transformed. She was, in her words, ‘myself again.’
What Is Magnesium and What Does It Do? The Complete Biology
Magnesium is the fourth most abundant mineral in the human body after calcium, phosphorus, and potassium. Total body magnesium in an adult is approximately 25 grams:
- 50 – 60% stored in bone
- 39% stored intracellularly (primarily in muscle)
- Less than 1% circulates in serum which is why serum magnesium is a poor reflection of total body stores
The Ten Critical Functions of Magnesium
- ATP synthesis: every molecule of ATP must be bound to magnesium to be biologically active. Without magnesium, cellular energy generation fails, explaining the profound fatigue of deficiency at a molecular level.
- Protein synthesis: required for ribosomal function and tRNA stability, the machinery of protein production
- DNA and RNA synthesis and repair: stabilises the double-helix structure of DNA; cofactor for DNA polymerase
- Neuromuscular transmission: acts as a natural calcium antagonist at the neuromuscular junction regulating calcium influx. Deficiency causes hyperexcitability: cramps, spasms, tremors, and in severe cases, seizures.
- Cardiac rhythm: stabilises the cardiac action potential by regulating potassium and calcium channels. Deficiency prolongs the QT interval (ECG changes) and predisposes to torsade de pointes, a life-threatening ventricular arrhythmia.
- Blood pressure: promotes vasodilation through vascular smooth muscle relaxation. Meta-analyses confirm magnesium supplementation lowers blood pressure in hypertensive patients.
- Insulin signalling: cofactor for insulin receptor tyrosine kinase. Deficiency impairs insulin signalling, worsening insulin resistance, creating a vicious cycle with diabetes.
- Vitamin D activation: both the hepatic and renal activation steps require magnesium-dependent enzymes. Low magnesium → Vitamin D supplementation fails.
- GABA receptor function and sleep: enhances GABA inhibitory activity in the brain — promoting relaxation and sleep. Deficiency causes anxiety, hyperarousal, and insomnia.
- Bone mineralisation: directly influences hydroxyapatite crystal formation. Deficiency found in 84% of post-menopausal women with osteoporosis in some studies.
💡 Clinical Insight: Magnesium is required to activate Vitamin D. Both the liver and kidney activation steps depend on magnesium-dependent enzymes. If a patient’s Vitamin D level is not rising despite consistent supplementation, check magnesium first. This is one of the most frequently missed interactions in nutritional medicine.
Magnesium Blood Test: How to Interpret Your Level And Why It Often Lies
This is one of the most important clinical principles in magnesium medicine: serum magnesium is a poor marker of true body magnesium status.
The kidneys defend serum magnesium within a tight range (0.75–0.95 mmol/L) by reabsorbing magnesium from urine when levels drop.
Serum magnesium can appear ‘normal’ even when intracellular and bone stores are significantly depleted.
The serum level only falls measurably when deficiency is severe enough to overwhelm this compensatory mechanism.
|
Serum Magnesium |
Status |
Clinical Implication |
|
> 0.85 mmol/L |
Normal |
Adequate serum level. Note: does NOT reflect intracellular or bone stores. Normal serum can coexist with significant cellular depletion. |
|
0.75–0.85 mmol/L |
Low-normal / Subclinical |
Symptoms may be present. Intracellular magnesium may already be depleted. Consider dietary optimisation or supplementation in symptomatic patients. |
|
0.60–0.74 mmol/L |
Mild deficiency |
Symptomatic. Oral supplementation indicated. Identify and address underlying cause |
|
0.40–0.59 mmol/L |
Moderate deficiency |
Significant symptoms. Risk of cardiac arrhythmia, hypocalcaemia, hypokalaemia. Oral supplementation; IV if symptomatic arrhythmia |
|
< 0.40 mmol/L |
Severe deficiency |
Medical emergency. Risk of seizures, torsade de pointes, tetany. IV magnesium sulphate urgently required |
Table 1. Serum magnesium level interpretation. Sources: NCBI StatPearls; Open Heart PMC; Cleveland Clinic.
More Accurate Tests for Magnesium Status
- 24-hour urinary magnesium: low urinary magnesium with low serum confirms deficiency and renal conservation. High urinary magnesium with low serum suggests renal wasting (diuretics, CKD).
- Magnesium loading test: IV magnesium given; urinary retention > 20% suggests deficiency. Considered the gold standard but not widely available.
- Red blood cell (RBC) magnesium: reflects intracellular magnesium more accurately than serum. Available in specialist labs.
💡 Clinical Insight: In a patient with
refractory hypokalaemia (potassium that will not correct despite supplementation) or refractory hypocalcaemia (calcium that will not correct despite supplementation), check magnesium first.
Magnesium deficiency is the most common reversible cause of both.
The kidney cannot conserve potassium or calcium effectively when magnesium is low. Correct the magnesium and the other electrolytes follow.
How Much Magnesium Do You Need Per Day?
The Upper Limit applies to supplemental magnesium only there is no upper limit for dietary magnesium from food. Excess food-source magnesium is safely excreted in urine.
|
Life Stage / Group |
RDA (mg/day) |
Upper Limit , Supplements Only (mg/day) |
|
Men 19–30 years |
400 mg |
350 mg |
|
Men ≥31 years |
420 mg |
350 mg |
|
Women 19–30 years |
310 mg |
350 mg |
|
Women ≥31 years |
320 mg |
350 mg |
|
Pregnant women 19–30 years |
350 mg |
350 mg |
|
Pregnant women ≥31 years |
360 mg |
350 mg |
|
Teen boys 14–18 years |
410 mg |
350 mg |
|
Teen girls 14–18 years |
360 mg |
350 mg |
Table 2. Magnesium RDA and supplemental Upper Intake Levels. Source: NIH Office of Dietary Supplements.
Magnesium Deficiency Symptoms: The 15 Warning Signs Most Doctors Miss
Magnesium deficiency is described as ‘silent’ because its symptoms are non-specific and overlap with dozens of other conditions. The result: it is investigated last, if at all.
|
System |
Mild to Moderate Deficiency |
Severe Deficiency (Hypomagnesaemia) |
|
Muscles |
Cramps, spasms, restless legs, fasciculations |
Carpopedal spasm, tetany, generalised seizures |
|
Cardiovascular |
Palpitations, mild ectopic beats |
Torsade de pointes (life-threatening), prolonged QT, sudden cardiac arrest |
|
Neurological |
Tingling, numbness, facial twitching, headache, migraine |
Seizures, coma, severe tremor, nystagmus |
|
Mental Health |
Anxiety, irritability, low mood, brain fog |
Depression, apathy, agitation |
|
Sleep |
Difficulty falling asleep, frequent night waking |
Chronic insomnia; disrupted REM architecture |
|
Metabolic |
Insulin resistance, fatigue after meals |
Worsening type 2 diabetes control; hypertension |
|
Bone |
Reduced bone density (Vitamin D activation impaired) |
Osteoporosis, magnesium deficiency found in 84% of post-menopausal women with osteoporosis |
|
Electrolyte disturbances |
Mild hypocalcaemia, mild hypokalaemia |
Refractory hypocalcaemia and hypokalaemia, impossible to correct without first fixing magnesium |
Table 3. Magnesium deficiency symptoms by severity. Sources: NCBI StatPearls; Open Heart PMC; Cleveland Clinic; Merck Manual.
Key Symptoms in Clinical Detail
1. Nocturnal Leg Cramps, The Most Common Presenting Complaint
Sudden, involuntary, excruciating contractions of the calf or foot muscles waking a person from sleep. It is caused by calcium-driven hyperexcitability of the neuromuscular junction when magnesium’s antagonistic effect is lost.
💡 Clinical Insight: Leg cramps have many causes: dehydration, circulatory problems, neurological disease, medication side effects. But in a patient with a diet low in magnesium-rich foods and perhaps on a diuretic or PPI, magnesium deficiency is an excellent first hypothesis to test with a therapeutic trial.
2. Insomnia and Non-Restorative Sleep
The biological basis for magnesium’s effect on sleep is well-established:
- Enhances GABA receptor sensitivity, the primary inhibitory neurotransmitter promoting relaxation
- Reduces cortisol, the stress hormone that disrupts sleep
- Regulates melatonin synthesis
- Reduces core body temperature promoting sleep onset
A 2024 RCT in Sleep Medicine: X found magnesium L-threonate improved both subjective sleep scores and objective sleep quality measures.
3. Anxiety and Psychological Symptoms
Magnesium modulates the hypothalamic-pituitary-adrenal (HPA) axis, the central stress response system. Deficiency leads to:
- Exaggerated cortisol responses to stress
- Lowered GABA activity
- Increased glutamate-driven neuronal excitation
The clinical result: anxiety, hypervigilance, irritability, and emotional dysregulation. Emerging RCT evidence supports magnesium supplementation for anxiety, particularly in those with documented deficiency.
4. Migraine and Chronic Headache
Magnesium deficiency causes cortical spreading depression, the electrophysiological event underlying migraine aura. Studies consistently show lower serum and red cell magnesium in migraine patients than controls. The German Neurological Society includes magnesium as a first-line preventive agent for migraine at 400–600 mg/day.
5. Cardiac Arrhythmias, The Most Dangerous Consequence
Magnesium is the cardiologist’s electrolyte. It is given intravenously worldwide for torsade de pointes, a form of polymorphic ventricular tachycardia that can degenerate into ventricular fibrillation and sudden death. IV magnesium sulphate is the first-line treatment.
At the subclinical level, deficiency is associated with:
- Atrial fibrillation
- Ventricular ectopics
- Prolonged QT interval
⚠️ Warning: Every patient with cardiac arrhythmia particularly those on loop diuretics should have their magnesium measured and optimised. This is simple medicine with potentially life-saving consequences.
6. The Vitamin D Connection, Why Your Supplement May Not Be Working
Both the hepatic and renal activation steps that convert Vitamin D to its active form require magnesium-dependent enzymes. If magnesium is deficient, Vitamin D supplementation may produce little or no rise in serum 25(OH)D.
💡 Clinical Insight: If a patient’s Vitamin D level is not rising despite consistent supplementation, check magnesium before increasing the Vitamin D dose. This combination is surprisingly common and completely reversible.
7. Refractory Hypokalaemia and Hypocalcaemia
The most practically important pearl in magnesium medicine: if a patient’s potassium or calcium will not correct despite supplementation, check the magnesium first. Magnesium deficiency impairs renal potassium conservation and suppresses PTH secretion, making hypokalaemia and hypocalcaemia impossible to correct until magnesium is replaced.
What Causes Magnesium Deficiency? Every Cause Explained
|
Cause |
Specific Cause |
Key Mechanism |
|
Dietary |
Low intake of whole grains, nuts, seeds, leafy greens |
Most common cause. Ultra-processed foods are stripped of magnesium. Soil depletion has reduced magnesium in crops by up to 30% since 1950 |
|
GI losses |
Chronic diarrhoea, IBD, short bowel syndrome |
Magnesium absorbed in small intestine; chronic GI losses deplete stores rapidly |
|
Alcohol |
Heavy or chronic alcohol consumption |
Alcohol increases urinary magnesium excretion dramatically; causes poor dietary intake and GI absorption |
|
Type 2 diabetes |
Poorly controlled diabetes / insulin resistance |
Hyperglycaemia causes osmotic diuresis — magnesium lost in urine. Low magnesium worsens insulin resistance — a vicious cycle |
|
Drug-induced |
Loop diuretics (furosemide, bumetanide) |
Most potent drug cause. Block magnesium reabsorption in the loop of Henle. Every patient on long-term loop diuretics needs monitoring |
|
Drug-induced |
Proton pump inhibitors (PPIs) |
Long-term PPI use (>1 year) reduces intestinal magnesium absorption via TRPM6 channel impairment. FDA black box warning since 2011 |
|
Drug-induced |
Calcineurin inhibitors (tacrolimus, cyclosporine) |
Cause renal magnesium wasting — near-universal in transplant patients on these drugs |
|
Drug-induced |
Cisplatin, aminoglycosides, amphotericin B |
Nephrotoxic drugs causing renal tubular damage and magnesium wasting. Cisplatin-induced hypomagnesaemia can be severe and long-lasting |
|
Renal losses |
CKD, renal tubular disorders |
Impaired tubular reabsorption of magnesium |
|
Increased demand |
Pregnancy, intense exercise, chronic stress |
Pregnancy increases demand for foetal development; exercise and stress increase urinary magnesium losses |
Table 4. Complete causes of magnesium deficiency. Sources: NIH ODS; NCBI StatPearls; Open Heart PMC; IJVNR 2025.
The PPI Problem – An FDA Warning Most Patients Never Heard
Proton pump inhibitors: omeprazole, lansoprazole, pantoprazole, esomeprazole are among the most widely prescribed drugs in the world. They carry a documented risk of clinically significant hypomagnesaemia with long-term use:
- Mechanism: PPIs impair intestinal magnesium absorption by disrupting the TRPM6 channel responsible for active magnesium transport
- The US FDA issued a drug safety communication in 2011 requiring all PPIs to carry a warning about hypomagnesaemia
- This warning is routinely overlooked in clinical practice
💡 Clinical Insight: Any patient on a PPI for more than 12 months should have annual serum magnesium monitoring. If hypomagnesaemia is confirmed, consider stepping down to an H2 blocker if clinically appropriate.
The Soil Depletion Factor
Intensive farming since the mid-20th century has significantly reduced the magnesium content of soil and therefore of crops. Studies comparing crop mineral content between 1940 and 2002 found reductions in magnesium of up to 30% in vegetables and cereals. Combined with the shift toward ultra-processed foods that strip away magnesium-rich bran and germ, modern populations are eating food that is fundamentally less magnesium-rich than previous generations.
Magnesium Deficiency Treatment: The Right Supplement Form Matters Enormously
Treatment is straightforward once the diagnosis is established but the choice of magnesium supplement form matters enormously. Not all magnesium supplements are equally absorbed, and buying the wrong one is a common and expensive mistake.
Which Magnesium Supplement Should You Take?
|
Form |
Bioavailability |
Best Used For |
|
Magnesium glycinate |
High |
Best overall choice. Well absorbed, gentle on stomach. Ideal for anxiety, sleep, muscle cramps, and long-term supplementation |
|
Magnesium malate |
High |
Excellent for muscle pain, fibromyalgia, fatigue. Malic acid supports energy production. Good daytime supplement |
|
Magnesium citrate |
Good |
Well absorbed, affordable, widely available. Mild laxative effect, useful in constipation. Most popular general supplement |
|
Magnesium L-threonate |
High (brain-specific) |
Crosses blood-brain barrier shown in 2024 RCT to improve sleep quality and cognitive function. Premium price but unique neurological benefit |
|
Magnesium taurate |
Good |
Combined with taurine, it supports cardiovascular health, blood pressure, and heart rhythm. Ideal for cardiac patients |
|
Magnesium oxide |
Only 4% |
Poorly absorbed. Mainly acts as laxative. Despite being the most commonly sold form, NOT recommended for correcting deficiency |
|
Magnesium sulphate (IV/IM) |
100% (parenteral) |
For medical emergencies: severe hypomagnesaemia, eclampsia, torsade de pointes. Hospital use only |
Table 5. Magnesium supplement forms — bioavailability and clinical applications. Sources: NIH ODS; Sleep Medicine X 2024; NCBI StatPearls.
The single most important principle: avoid magnesium oxide unless you specifically need its laxative effect. Despite being the most common form sold in pharmacies, its absorption rate is only approximately 4%.
For correcting deficiency, magnesium glycinate is the gold standard.
Treatment Protocol by Clinical Scenario
|
Clinical Scenario |
Treatment |
Monitoring & Duration |
|
Mild dietary deficiency |
Magnesium glycinate or citrate 200–400 mg elemental/day |
Recheck serum magnesium at 8–12 weeks. Address dietary cause long-term |
|
Moderate symptomatic deficiency |
Magnesium glycinate or malate 400–600 mg/day in divided doses |
Symptoms improve within 2–4 weeks. Continue 3–6 months to replenish intracellular stores |
|
Refractory hypokalaemia or hypocalcaemia |
Correct magnesium FIRST, oral or IV. Potassium and calcium cannot be corrected until magnesium is replenished |
Monitor all three electrolytes together |
|
Severe deficiency / cardiac arrhythmia |
IV magnesium sulphate 1 – 2 g over 5 – 60 minutes. ECG monitoring required |
Repeat serum Mg at 4–6 hours. Transition to oral once stable. |
|
Eclampsia / pre-eclampsia |
IV magnesium sulphate 4 – 6 g loading dose, then 1 – 2 g/hour. Standard obstetric protocol |
Monitor reflexes, urine output, respiratory rate. Antidote: IV calcium gluconate |
|
Long-term loop diuretic therapy |
Oral magnesium 200 – 400 mg/day routinely |
Annual serum magnesium monitoring minimum |
|
PPI-induced hypomagnesaemia |
Oral magnesium supplementation. Review PPI indication, switch to H2 blocker where possible |
Magnesium may not fully normalise while PPI continues |
|
Diabetes / insulin resistance |
Magnesium glycinate 300 – 400 mg/day. Optimise glycaemic control |
Pooled RCT analysis shows magnesium supplementation improves insulin sensitivity |
Table 6. Magnesium treatment protocol. Sources: NCBI StatPearls; Open Heart PMC; Cleveland Clinic.
Practical Supplementation Tips
- Take with food: absorption is better with meals; GI side effects are reduced
- Split the dose: 200 mg twice daily is better than 400 mg once. It improves absorption and reduces osmotic diarrhoea
- Take glycinate or L-threonate in the evening: GABA-enhancing effects support sleep when taken 1–2 hours before bed
- Do not take with calcium supplements: Separate by at least 2 hours. Calcium and magnesium compete for absorption
Recovery Timeline
|
What Improves |
Timeline After Starting Treatment |
|
Muscle cramps |
1–2 weeks |
|
Sleep quality |
2–4 weeks |
|
Anxiety and mood |
4–8 weeks |
|
Blood pressure |
8–12 weeks |
|
Serum magnesium normalises |
Weeks; intracellular stores take 3–6 months to replenish fully |
Table 7. Magnesium deficiency recovery timeline. Source: Clinical experience + NCBI StatPearls.
Magnesium Toxicity, Can You Take Too Much?
- From food: No, the kidneys efficiently excrete excess dietary magnesium
- From supplements: the upper limit of 350 mg/day supplemental applies. Exceeding this chronically causes diarrhoea, nausea, and in severe overdose lethargy, low blood pressure, respiratory depression
- Kidney disease: CKD patients must use only under medical supervision impaired kidneys cannot excrete excess magnesium
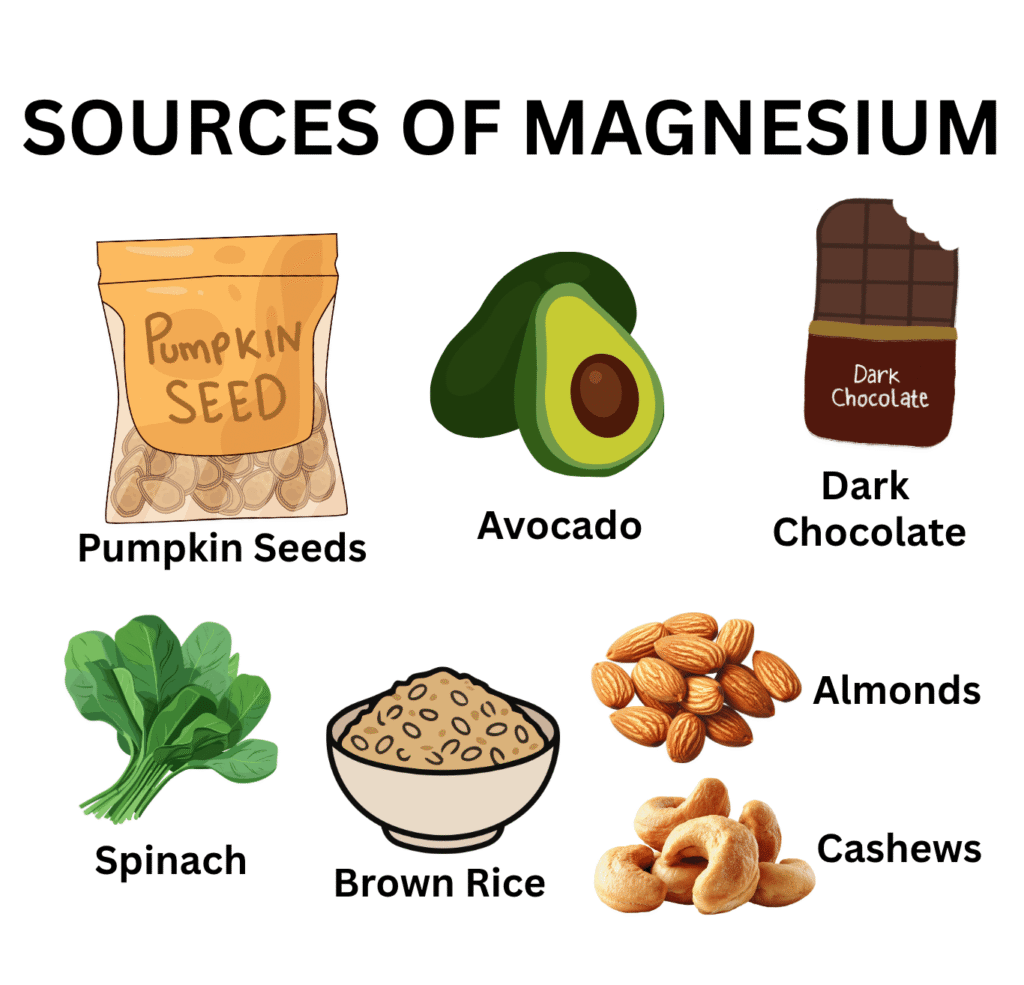
Best Food Sources of Magnesium
The richest dietary sources are the foods most absent from Western ultra-processed diets: nuts, seeds, whole grains, dark leafy vegetables, and legumes.
|
Food Source |
Serving Size |
Magnesium (mg) |
|
Pumpkin seeds (roasted) |
28 g (1 oz) |
156 mg ✦ Highest per serving |
|
Almonds |
28 g (1 oz) |
80 mg |
|
Spinach (boiled) |
½ cup (~90 g) |
78 mg |
|
Cashews |
28 g (1 oz) |
74 mg |
|
Dark chocolate (70–85% cocoa) |
28 g (1 oz) |
64 mg |
|
Black beans (cooked) |
½ cup (~86 g) |
60 mg |
|
Edamame (cooked) |
½ cup (~75 g) |
50 mg |
|
Peanuts (roasted) |
28 g (1 oz) |
49 mg |
|
Brown rice (cooked) |
½ cup (~98 g) |
42 mg |
|
Avocado |
½ medium |
29 mg |
|
Banana |
1 medium |
32 mg |
Table 8. Top dietary sources of magnesium. Source: NIH ODS / USDA FoodData Central. Adult men RDA = 420 mg/day; women = 320 mg/day.
🍫 Practical Tip: A handful of mixed nuts daily (almonds, cashews, pumpkin seeds) contributes 80–150 mg of magnesium. Dark chocolate (70–85% cocoa) is a genuine clinical recommendation, not just a pleasure. And switching from white rice to brown rice doubles the magnesium content per serving at zero extra cost.
How to Prevent Magnesium Deficiency: Strategies for Every Risk Group
For the General Population
- Eat nuts, seeds, legumes, whole grains, and dark leafy greens daily
- Choose whole grain over refined grain products magnesium is in the bran and germ, which refining removes
- Limit ultra-processed food consistently low in magnesium and displaces whole foods from the diet
- Limit alcohol, even moderate regular drinking increases urinary magnesium losses.
For High-Risk Groups
|
Population Group |
Recommended Daily Dose |
Key Reason |
|
General adult (dietary gap) |
200–400 mg elemental/day |
Stay within 350 mg/day supplemental upper limit |
|
Type 2 diabetes patients |
300–400 mg/day |
Vicious cycle: diabetes depletes magnesium; low magnesium worsens diabetes |
|
Loop diuretic users |
200–400 mg/day routinely |
Furosemide causes massive urinary magnesium losses with every dose |
|
Long-term PPI users |
Monitor; supplement if deficient |
FDA black box warning: annual serum magnesium testing mandatory |
|
Cardiac patients / arrhythmia |
Magnesium taurate 200–400 mg/day |
Magnesium stabilises cardiac action potential |
|
Sleep problems / anxiety |
Magnesium glycinate 200–400 mg at bedtime |
GABA-enhancing effects support sleep onset and reduce anxiety |
|
Migraine sufferers |
Magnesium citrate 400–600 mg/day |
German Neurological Society: first-line migraine preventive agent |
Table 9. Magnesium supplementation recommendations by population group. Sources: NIH ODS; Open Heart PMC; Cleveland Clinic.
Magnesium vs Potassium vs Calcium Deficiency: How to Tell Them Apart.
These three electrolyte deficiencies overlap significantly and frequently occur together. The critical clinical rule: magnesium almost always needs to be corrected first, because low magnesium prevents potassium and calcium from being retained.
|
Feature |
Magnesium Deficiency |
Potassium Deficiency |
Calcium Deficiency |
|
Key symptoms |
Cramps, anxiety, insomnia, arrhythmia |
Cramps, weakness, constipation, arrhythmia |
Muscle cramps, tetany, dental decay, numbness |
|
Cardiac risk |
Torsade de pointes, life-threatening |
Atrial fibrillation, ventricular arrhythmia |
Less direct, mainly via PTH dysregulation |
|
Key diagnostic test |
Serum magnesium (limited sensitivity) |
Serum potassium |
Serum calcium + PTH |
|
Critical interaction |
Low Mg → refractory low K and low Ca |
Low K often caused by low Mg, fix Mg first |
Low Ca may be caused by low Mg → fix Mg first |
|
Common drug causes |
Loop diuretics, PPIs, cisplatin |
Loop diuretics, laxatives |
Loop diuretics, anticonvulsants |
|
Treatment rule |
Always correct FIRST if other electrolytes are also low |
Will not correct until magnesium is fixed |
Will not correct until magnesium is fixed |
Table 10. Comparative guide — Magnesium vs Potassium vs Calcium deficiency. Source: Clinical experience + NCBI StatPearls; NIH ODS.
Frequently Asked Questions About Magnesium Deficiency
Related Articles on MedBeaconHub.com
- Nutritional Deficiency Diseases: A Doctor’s Complete Guide (Pillar Article)
- Vitamin D Deficiency: Why Magnesium Is the Missing Key to Your Supplement Not Working
- Calcium Deficiency: The Magnesium-Calcium Relationship Explained
- Potassium Deficiency: Why Correcting Magnesium Comes First
- Iron Deficiency Anaemia: Complete Clinical Guide
- Vitamin B12 Deficiency: Another Cause of Fatigue and Neurological Symptoms
References and Authoritative Sources
- NIH Office of Dietary Supplements — Magnesium Fact Sheet for Health Professionals
- NCBI StatPearls — Hypomagnesaemia
- PMC Open Heart — Subclinical Magnesium Deficiency: A Principal Driver of Cardiovascular Disease
- IJVNR 2025 — Global Dietary Magnesium Deficiency: Prevalence, Causes, Health Consequences
- Sleep Medicine: X 2024 — Magnesium L-Threonate Improves Sleep Quality (RCT)
- Frontiers in Nutrition 2025 — Magnesium L-Threonate: Randomised Double-Blind Placebo-Controlled Trial
- Nutrients 2025 — Magnesium and Migraine (Dominguez et al.)
- Cleveland Clinic — Hypomagnesaemia (Low Magnesium)
- Merck Manual Professional Edition — Hypomagnesaemia
- PMC Nutrients 2025 — Magnesium Depletion Score as an Indicator of Health Risk (Tufts University)